Research Article
Prevalence of Smoking, and its Relationship with Depression, and Anxiety in a Sample of Iranian High School Students
Khademalhosseini Z, Ahmadi J, and Khademalhosseini M*
*Substance Abuse Research center and Research Center for Psychiatry, Shiraz University of Medical Sciences, Shiraz, Iran
Corresponding author
Khademalhosseini Mitra, Substance Abuse Research center and Research Center for Psychiatry, Shiraz University of Medical Sciences, Shiraz, Iran, Tel: +9809177056089; E-mail: khadem82@gmail.com
Received Date: 17th October 2014
Accepted Date: 17th February 2015
Published Date: 20th February 2015
Citation
Khademalhosseini Z, Ahmadi J, Khademalhosseini M (2015) Prevalence of Smoking, and its Relationship with Depression, and Anxiety in a Sample of Iranian High School Students. Enliven: Pharmacovigil Drug Saf 2(1): 001.
Copyright
@ 2015 Khademalhosseini Mitra.This is an Open Access article published and distributed under the terms of the Creative Commons Attribution License, that permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Psychiatric disorders, like anxiety and depression, are risk factors for drug abuse and smoking behavior. The purpose of this survey was to determine the prevalence of smoking, depression and anxiety and their relationship among school age students. This cross-sectional survey was done on 1020 high school students (male and female) recruited randomly and DSM-IV interview was done by researchers. A psychiatry resident accompanied by 3 last year medical students interviewed with students and a questionnaire containing demographic , anxiety and depression questions was filled simultaneously. The obtained data were analyzed using SPSS16. 50% of the students were female and the remainder male. 277 students (27.2%) were in the first year, 242 (23.7%) in the second year and 501 (49.1%) in the third year of high school. 55 students (5.4%) were smoker and used cigarette , water pipe (hobble bobble) and pipe.183 students (18%) had anxiety and stress symptoms (mild, moderate , sever). The 29 smoker students (2.84%) had anxiety. 144 students (14.1%) had depression (mild, moderate, sever) and 23 smoker students (2.25%) had depression symptoms. There was no significant correlation between smoking and anxiety and depression symptoms among school age students. As conclusion, we hypothesized that smoking may increase the tendency to depression and anxiety in high school students. Although the above results didn't demonstrate any significant correlation between these three issues, school counselors and teachers need to be informed about the prevalence of problematic behaviors associated with smoking and it would be necessary to develop smoking prevention programs for adolescents, while taking the psychological factors such as depression and anxiety and school and family atmosphere into account.
Keywords
Smoking; Water pipe; Cigarette; Pipe; High school; Depression; Anxiety
Abstract
Psychiatric disorders, like anxiety and depression, are risk factors for drug abuse and smoking behavior. The purpose of this survey was to determine the prevalence of smoking, depression and anxiety and their relationship among school age students. This cross-sectional survey was done on 1020 high school students (male and female) recruited randomly and DSM-IV interview was done by researchers. A psychiatry resident accompanied by 3 last year medical students interviewed with students and a questionnaire containing demographic , anxiety and depression questions was filled simultaneously. The obtained data were analyzed using SPSS16. 50% of the students were female and the remainder male. 277 students (27.2%) were in the first year, 242 (23.7%) in the second year and 501 (49.1%) in the third year of high school. 55 students (5.4%) were smoker and used cigarette , water pipe (hobble bobble) and pipe.183 students (18%) had anxiety and stress symptoms (mild, moderate , sever). The 29 smoker students (2.84%) had anxiety. 144 students (14.1%) had depression (mild, moderate, sever) and 23 smoker students (2.25%) had depression symptoms. There was no significant correlation between smoking and anxiety and depression symptoms among school age students. As conclusion, we hypothesized that smoking may increase the tendency to depression and anxiety in high school students. Although the above results didn’t demonstrate any significant correlation between these three issues, school counselors and teachers need to be informed about the prevalence of problematic behaviors associated with smoking and it would be necessary to develop smoking prevention programs for adolescents, while taking the psychological factors such as depression and anxiety and school and family atmosphere into account.
Introduction
Greatest preventable cause of death entire the word is related to Smoking and Tobacco use [1,2]. Although smoking and its related problems are a great public concern, the rate of smoking is still high and about a quarter of the population smoke [3]; each year about 5 million people die from smoking -related conditions [1].
Many studies have shown that psychiatric disorders, like anxiety and depression, are the risk factors for drug abuse and smoking behavior [4-7]. This study aimed to investigate the prevalence of smoking and anxiety and depression among school students and allows finding out the relationship between these three issues. School environment is a potential place for initiating smoking and drinking because a great number of the youth spend many times together and are influenced by other students’ behavior and specially their teachers whereas they are in a critical age period. As schools are often the first line for identification of potential life-threatening behaviors, school-based health professionals need to be aware of measures and procedures for the assessment of smoking, depression, and anxiety [8].
Methods
In a cross-sectional study, 1020 high school students from 4 different districts of Shiraz in the south of Iran (male and female) were selected via cluster random sampling from 10 high schools to assess anxiety and depression levels and their relationship with smoking among students. Three last year medical students with supervision of a psychiatry resident interviewed with students privately based upon DSM-IV criteria. During the interview, they determined and recorded mental health and smoking status of students. As well, demographic, anxiety and depression questionnaires were completed. The questionnaire was approved by the college authorities as there was no formal research ethics committee. The investigators spent about 20 minutes for each student for diagnosing anxiety and depression. Before the interview, the goal of study was explained for the students and they were encouraged to participate in the study and were motivated to express their experiences. The students gave their informed verbal consent to participate in the study and were ensured about the confidentiality. They were asked not to say anything about their names, family or student number. The pilot study of the questionnaire was performed on 30 high school students and favorable results were obtained. The gathered data were analyzed using SPSS, version16. Descriptive statistics and Chi-square test were used to analyze the data.
Definitions
Degree of Depression According to Sign and Symptoms
Mild: Decreased mood, symptoms of anxiety, and increased symptoms in the afternoon, without suicidal idea.
Moderate: Decreased activity, depressed mood, agitation, decreased energy, and decreased concentration, sense of guilt, hypochondriacs, sleep disturbance, depersonalization symptoms, decreased appetite, decreased sexual activities. Severe: nihilistic delusions and auditory and visual hallucinations.
Frequency of Smoking
Occasional: Once per month or less.
Frequent: Once per week or less.
Regular: Twice per week or more.
Dependent: Withdrawal symptoms after abstinence.
Abuser: Dysfunction symptoms after abstinence.
Economical Status
Low: Less than 3000000 RILS per months
Moderate: 3000000 -1000000RILS per months
High: More than 10000000 RILS per months
Results
The sample consisted of 1020 high school students. The gender was evenly distributed (50% male, 50% female). The students’ mean age was 16.3 (SD: 4.23), (range: 13-19 years). The mean age of the female students was 15.9 (SD: 3.38) and that of males was 16.7 (SD: 4.61). Frequency and demographic data are displayed in Table 1.
| variable | Frequency(%) | |
| Age | ||
| 13-15 | 249(24.40) | |
| 15-17 | 230(22.50) | |
| 17-19 | 540(53.00) | |
| Sex | ||
| Male | 510(50) | |
| Female | 510(50) | |
| Educational level | ||
| 1thyear | 277(27.2) | |
| 2thyear | 242(23.7) | |
| 3thyear | 501(49.1) | |
| Economic level | ||
| Low | 140(13.7) | |
| Moderate | 807(79.1) | |
| high | 62(6.1) | |
Table 1. Demographic variables
1013 students (99.3%) didn’t use cigarette. 977 students (95.8%) didn’t use water pipe and 1015 students (99.5%) didn’t use pipe. 55 students (5.4%) were smoker and used cigarette and its derivates, water pipe (hobble bobble) and pipe. 183 students (18%) had anxiety and stress symptoms (mild, moderate , sever) and 144 students (14.1%) had depression (mild, moderate, sever). Table 2 shows the prevalence of smoking (cigarette, water pipe, and pipe) and anxiety and depression among students. Prevalence of anxiety and depression was significantly higher in females (P value < 0.05). Prevalence of anxiety decreased significantly in third year students (P value < 0.05). In the 1st year students, depression was seen more than the 2nd and 3rd year. Prevalence of depression was significantly higher in students with lower economical status (p value < 0.01). With increase in age, cigarette and pipe smoking increased as well but not significantly. Male students smoked water pipe more than females significantly (p < 0.01). 3rd year students smoked less water pipe and pipe and the correlation was significant (p < 0.05). In general, the prevalence of smoking (cigarette, water pipe, and pipe) in moderate economic level was more. Of 55 smoker students, 29 (2.84%) had anxiety and 23 smoker students (2.25%) had depression symptoms. 13 students (1.27%) had the three mentioned conditions simultaneously, and 100 students (9.8 %) had both depression and anxiety. There was no significant correlation between smoking and anxiety and depression symptoms among school age students. Graphs A and B show the relationship among smoking, depression and anxiety.
| variable | Frequency(%) | |
| Anxiety | ||
| no | 836(82.0) | |
| Mild | 107(10.5) | |
| Moderate | 54(5.3) | |
| sever | 22(2.2) | |
| Depression | ||
| No | 867(85) | |
| Mild | 98(9.6) | |
| Moderate | 37(3.6) | |
| sever | 9(.9) | |
| Cigarette smoking | ||
| No | 1013(99.3) | |
| Occasional | 2(.2) | |
| Frequent | 2(.2) | |
| regular | 3(.3) | |
| Waterpipe(hobblebobble) | ||
| No | 977(95.5) | |
| Occasional | 31(3) | |
| Frequent | 2(.2) | |
| Regular | 8(.8) | |
| dependent | 2(.2) | |
| Pipe | ||
| No | 1015(99.5) | |
| Occasional | 5(.5) |
Table 2. Non- demographic variables
Discussion
This study examined the prevalence of smoking, depression and anxiety and their relationship with each other in high school students and compared them across genders, age, grade of high school and economic background.
Smoking and Tobacco Derivate Use
Although in many developed countries the prevalence of smoking and tobacco use in adolescents has been measured, in many developing countries, statistics, measures and predisposing factors and related concerns about smoking are a good field of study for researchers [9]. In Iran besides cigarette and pipe, there is a traditional tobacco derivate named “ghalyan”, which originates from ancient Persia and India [10]. In English, it is called “hobble-bobble or water pipe” and its use is very common among adolescents in Iran. In this study "smoking" refers to cigarette, pipe and water pipe. The prevalence of Tobacco use from 1994 to 2000 in Iranian population has had an upraise pattern both among men (26% to 29%) and women (1.4% to 5.3%), especially in youths [11-16]. In the sample group of this study, 55 school age students (5.39%) were smoker with a higher prevalence in boys than in girls (7.84 vs. 2.94); this means 1013 students were non-smoker, neither now nor in the past. According to previous surveys of adolescents in Iran, some of them reported that the prevalence of smoking and tobacco use is 19.4% [17] and 28.9% [18] among smoking students, but other studies estimated its range from 2.5% to 14.3% [19,20]. In a study, the prevalence of tobacco use based on serum cotinine level was 12.5% [21]. However with the increase in age, cigarette and pipe use increased too but the correlation wasn’t significant. Jafarabadi A et al. [22] and Kelishadi et al. [20] in their studies in Iran were in the same line with our results. They found that as age increases, the odds of smoking increases by 27% of our study, smoking water pipe and age had any significant correlation. The rate of cigarette use among the students was significantly lower than the results of Ahmadi et al.’s in 2003 [23].
Many surveys confirm the results of our study about higher smoking prevalence in males than females. (24 - 26) 2.94% of females and 7.84% of males was smoker. Sex and water pipe smoking had a significant correlation (P < 0.01); thus, males smoked water pipe and pipe more than females. As to cigarette, females with a shade and nuance, smoke more than males but the link wasn’t significant. Roohafza et al. [27], in their investigation, reported that males smoke water pipe and cigarette more than females; it was a different result. Due to lack of studies about smoking in adolescents in Iran, and because many of them are self reports, the exact estimate for prevalence rate and comparison is difficult. According to researches done all over the world , it should be noticed that not only in most of the investigations done in Iran but in those conducted in other countries both developed and developing countries , the prevalence of adolescents’ smoking is higher than this study and it ranges from 14.2% to 39%, for example Spain [28], Tunisia [29], Italy [30], France [31], Chile [32], China [33], Australia [34], USA [35], Finland [36], Japan [37], Saudi Arabia [38], and Canada [39]. Although researchers in this survey were sure about students’ reliance on the study and illustrated them the aim and confidentiality aspects, the interview may interfere in the results. Strict and strong roles and regulations in high schools in Iran, social and familial stigma of smoker adolescents, and cultural background could be other affecting factors. In the present study, out of 510 female students, 2.94% were smoker and most of them (1.96%) use water pipe. These percentages, in comparison with other studies in other areas of the world, are low but are similar to the results on serum cotinine level in Iranian teenagers [21]. Third year students used water pipe and pipe lower than first and second year students and the relationship was significant (p < .01). Considering the high load of school works in last year of high school and probable changes in students’ information about disadvantages of smoking via educational courses or special advices by teachers in high schools, this result could come true. In two extreme of economical status innuendo low and high degrees, prevalence of tobacco use especially water pipe was very low and most of smoker students were in average level. Whereas in most investigations all over the world, tobacco use is inversely related to social and economical position (40 – 46). However most of the students were in moderate level, but further studies are needed for uncompromising reasons. According to the results, Occasional tobacco users were majority of smokers and among students anybody wasn't abuser fortunately. Summing up, the findings of this study like another studies in Iran showed low prevalence of smoking among adolescences, particularly in female group [47,11] and we can state that tobacco use especially in women is yet low in Iran than most of other countries.
Smoking and Depression
Recently many appreciable inspections have found out the relationship between psychological conditions like depressive symptoms and smoking [49,50]. Indeed in behavioral diseases clinics most smokers have some degrees of depression. [51] According to Co morbidity researches, heavy smoking and depression are related to each other [52-55,5]. In this study, 144 students (14.1%) had different degrees of depression and majority (98%) had mild depression.
like other studies [56,57] depression was more common in female students than male (p< .01). Age had not marked interdependence with depressive symptoms. In first year students depression was more than second and third year students. Indeed encounter with new environment and people, embody teachers and other students and poor coping skills, would legitimize this, but additional studies are necessary.
In Low economical state group, more students had depression and correlation was significant (p< .01). In contrast to previous findings [58] and in support of another studies [59], we found that the link between smoking and depression is not strong and just 23 of students (2.25%) were smoker and had depression contemporary. Although statistical analysis showed no relation between depression and smoking in study group but could not ignore these numbers of smoking students who suffered depression. Their quality of life, educational progress and interpersonal relationship are so important that counselors and physicians peruse these two issues in student's history and give related council and treatments.
Smoking and Anxiety
As well as focus on coexistence of depression and substance use and smoking , also many studies have paid attention to the anxiety disorders recently [60-63] although the cause of co occurrence of these conditions is not well understood [64] but there is evidence that tobacco use increases the risk of anxiety disorders [59,63]. Mykletun A et al. demonstrated that anxiety is more correlated with smoking than depression [59].
The results of this survey showed that 183 students (18 %) had anxiety. Bernstein et al. and Boyd et al. estimated anxiety prevalence range from 4.0% to 25.0%, with an average rate of 8.0% [65,66]. They declared that the prevalence could be underestimated when anxiety among adolescents goes undiagnosed because of the internalized nature of disease [67]. In female group 69 girls (22.35%) had anxiety symptoms that was more than male. any expressive relation between sex and anxiety didn't find . in former studies women were two fold as likely as males developed anxiety disorders [56,68,69]. with increasing in age anxiety decreased in a sluggish pattern. Students in 1st year had more anxiety than higher stages that is in opposite point of Peterson et al. and Malkin et al. study [70,71]. No relation between anxiety and economical state was seen that is a different result in comparison with some other studies. Deb et al. in their paper explained that the mean value of anxiety for teenagers in middle socio-economic class (30.07), was higher than lower (28.62) and higher (23.60) socio-economic class [72]. 29 students (2.84%) had anxiety and contemporary used tobacco derivates. those who used water pipe had more anxiety. In a remarkable Co morbidity survey in 1,507 adolescents in a frame of combined cross-sectional and longitudinal design Brown et al. [73] demonstrated a debilitated link between tobacco use and anxiety. Beside this study Costello et al. [74] found that teenagers with anxiety are prone for nicotine dependence but the results were not statistically significant. As well as named researches, many other studies [7] tried to again and again examine mentioned association and explore that tobacco use might be different among the anxiety disorders and nicotine dependent individuals have more anxiety symptoms. In opposition to studies suggested that anxiety has association with smoking and nicotine dependence [59,63] and like the results in a survey was done by Johnson et al. [60], we found that there is no link between anxiety and smoking and may are previous studies under special circumstances and in different census society be distributable. Of course number of study group is important and in small sample size the exact results were interfered. More investigations should scrutinize for proving the association in greatest sample size.
General Discussion
Many recently studies have shown in adult smokers that mental and intellectual haleness, High degree depression and anxiety and tobacco use are related to each other. Indeed psychiatric patients had higher smoking rate than normal population [49-53,55,57-64,69,73,74]. earlier surveys in nicotine dependent people reported substantial high rate in mood and anxiety disorders and the prevalence of 21.1for mood disorders and 11.1% for anxiety disorders [75], that is higher than normal population (9.2%). Except in adults, Depression and anxiety are commonly reported issues among college-aged populations and much psychiatrist use Anxiety and Depression as dependable gauge for appraisal of mental health in people [76]. Three noteworthy studies in USA [71,77] and Australia [78] conducted in teenage population, indicated a remarkable association between depression and anxiety symptoms and smoking and twice increment in the risk for regular smoking and accretion in both frequency and quantity and morbidity related conditions and the link was particularly evident in the youngest teenage group. In some studies co occurrence of poor mental health and smoking and basic scientific mechanisms were illustrated. The literature seems to suggest that the process may be reciprocal [6]. According to them smoking (nicotine) causes neurochemical changes in body that begets mental disorder symptoms or because of poor mental health, trend to smoking for relieve of feelings and adverse symptoms, become raised [53,79,80]. Also Mental health disorders can cause low self-esteem, poor coping strategies and neuroticism and substance use is a way for coping with psychological distress and adverse symptoms of anxiety or depression [7,81,82]. It shouldn’t be forget that genetic or environmental factors directly or indirectly increase the risk of having both conditions [73,80]. Although many previous studies [62] tried to illustrate relationship between smoking and anxiety and depression in patients, but many of them couldn’t find any remarkable relationship between degree of dependence to drug and Depression and anxiety [58].
Our results suggest that in 13 students, causality relation exist and 1.27% of students had three mentioned condition simultaneously, and 100 students (9.8 %) had both depression and anxiety. whereas Mykletun et al. showed that Anxiety and depression are commonly co morbid and 5.9% adolescence had both anxiety and depression [83]. Building upon this work such as other studies Students who used cigarette, water pipe and pipe had higher rates of depression and anxiety but it wasn’t statistically significant maybe because of lower rates of addiction in our students, these results was not statistically significant. Summing up, it can be state that among studies related these issues; differences can result from the different conditions, instruments, and differences in the number and structure of the study group. In every research, there are some limitations that can result in restriction of outcomes and couldn’t generalize them to a bigger group. Hence we can’t generalize the results of this study to the other students and adolescents, additionally smoking are a very multi factorial subject that familial, social and economical status, culture, education and availability are other factors which related to it. So, each community needs specific study. The most cardinal limitation of this study was that it was cross-sectional, which doesn't let us, to interpret outcomes base upon experimental observation and doesn’t allow us to investigate that how causal relationship cross a longer period happen. Current investigation was base an interview with students, which is under influence of potential reporting errors and lack of enough trust to confidentiality aspects. Whatsoever the sample-size is larger, researchers have more power to detect every small relation, and error rate diminishes and generalization is easier. The data for this study were collected in students studied in 10 high school in Shiraz city in south of Iran therefore can’t generalize the results not only the whole world but also Iran.
Suggestions
With regard to previous researches results, teenagers smoke since 16 years old continue it for 16-20 years [84] and with take notice to diminution in physical and educational performance in school, as well as probability of developing smoking related diseases in future [18], planned preventive programs in society and schools can be useful in smoking imitation and scale down the rate of it. High school age is a time of emotional consternation and students are more under influence of social hazards than other life periods. Smoking and related problems are important social concerns and Preventing youth from starting to smoke or delaying initiation should be a public health priority. Educationists as well as teachers and parents should try to understand the root causes of trend to smoking and need to be made aware of the prevalence and the problematic behaviors associated with it. Assumption of specific disciplines and suitable regulations can limit environmental factors and peer influence in school [86-87]. tobacco control strategies and Perform policies for control of smoking in society by government , like reducing smoking in movies [87,88] and advertisements , production of alarming programs by media , cognizance of demographic factors and life style training and improving personal skills by counselors for "saying no" [22] against extrinsic and intrinsic motivating factors can be helpful.
In synopsis we should state that: for restriction of problems related to smoking and anxiety and depression, we need an integrative approach, collaboration and coordination of many politic and social services, student life professionals, academic advisers, career counselors, judicial and disciplinary affairs staff, and security services personnel and all mentioned services should consider scientific results in literature and rely and come along them.
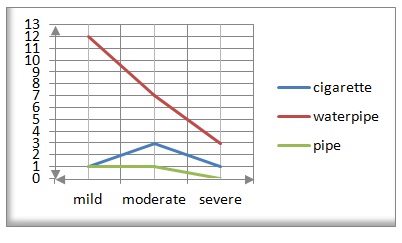
Figure 1 Relationship of anxiety and smoking
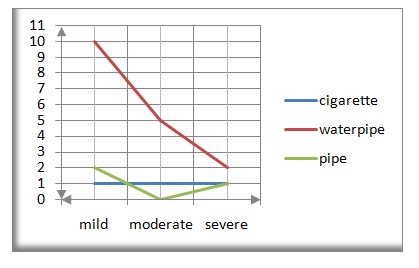
Figure 2 Relationship of depression and smoking
Conclusions
The aim of the study presented here was to investigate and quantify prevalence of smoking, depression, anxiety and their associations and conjunction spot. Although The results of this study, showed that there is not statistically relationship between smoking and anxiety and depression in high school students but also provide evidence of their prevalence in south of Iran and helps health policy makers for conduction new and effective programs.
References
- Murray CJ, Lopez AD (1997) Alternative projections of mortality and disability by cause, Global Burden of Disease Study. Lancet 349: 1498-1504.
- Centers for Disease Control and Prevention (CDC) (1994) Medical care expenditures attributable to cigarette smoking - United States. MMWR Morb Mortal Wkly Rep43: 469-472.
- Centers for Disease Control and Prevention (CDC) (2001) Youth tobacco surveillance: United States. MMWR CDC Surveill Summ 50: 1-84.
- Brewer DD, Catalano RF, Haggerty K, Gainey RR, Fleming CB (1998) A Meta analysis of predictors of continued drug use during and after treatment for opiate addiction. Addiction 93: 73-92.
- Breslau N, Kilbey M, Andreski P (1991) Nicotine dependence, major depression, and anxiety in young adults. Arch Gen Psychiatry 48: 1069-1074.
- Deykin EY, Levy JC, Wells V (1987) Adolescent Depression, Alcohol and Drug Abuse. Am J Public Health 77: 178-182.
- Morrell HER, Cohen LM (2006) Cigarette Smoking, Anxiety, and Depression. Journal of Psychopathology and Behavioral Assessment 28: 4.
- Ryu EJ, Choi KS, Seo JS, Nam BW (2004) The relationships of Internet addiction, depression, and suicidal ideation in adolescents. Taehan Kanho Hakhoe Chi 34: 102-110.
- Surani NS, Shroff HP (2012) Mass media exposure to tobacco messages among secondary school children in Mumbai. Indian J Public Health 56: 159-162.
- World Health Organization Regional Office for the Eastern Mediterranean (2008) A strategy for health promotion in the Eastern Mediterranean Region 2006-2013.
- Boshtam M, Rafiei M, Sarraf Zadegan N, Asgary S, Khalili A (2000) Smoking prevalence and its combination with some cardiovascular risk factors. Acta Medica Iranica 38: 115-120.
- Ahmadi J, Khalili H, Jooybar R, Namazi N, Mohammadagaei P (2001) Prevalence of cigarette smoking in Iran. Psychol Rep 89: 339-341.
- Ahmadi J, Hasani M (2003) Prevalence of substance use among Iranian high school students. Addict Behav 28: 375-379.
- Ahmadi J, Hasani M (2003) Prevalence of substance use among Iranian high school students. Addict Behav 28: 375-379.
- Ahmadi J, Maharlooy N, Alishahi M (2003) Substance abuse: prevalence in a sample of nursing students. J Clin Nurs 13: 60-64.
- Ahmadi J, Benrazavi L, Ghanizadeh A (2001) Substance Abuse among Contemporary Iranian Medical Students and Medical Patients. J Nerv Ment Dis 189: 860-861.
- Ahmadi J, Khalili H, Jooybar R, Namazi N, Aghaei PM (2001) Cigarette smoking among Iranian medical students, resident physicians and attending physicians. Eur J Med Res 6: 406-408.
- Heidari GR, Amini S, Maleki E, Hosseini M, Masjedi R (2005) Prevalence of light smoking and attitudes and knowledge of smokers toward that in Tehran in 2003. J Med Coun IR Iran 24: 224-231.
- Alireza Ayatollahi S, Mohammadpoorasl A, Rajaeifard A (2005) Predicting the three stages of smoking acquisition in the male students of Shiraz's high schools in 2003. Nicotine Tob Res64: 10-15.
- Ayatollahi SR, Mohammadpoor A, Rajaee AR (2003) Determination of the prevalence of stages in cigarette smoking and its correlates in grade-10 male students in Shiraz. J Mazandaran Uni Med Sci 43: 71-84.
- Kelishadi R, Ardalan G, Gheiratmand R, Majdzadeh R, Delavari A, et al. (2006) Smoking behavior and its influencing factors in a national-representative sample of Iranian adolescents. Prev Med 42: 423-426.
- Sarraf-Zadegan N, Boshtam M, Shahrokhi S, Naderi GA, Asgary S, et al. (2004) Tobacco use among Iranian men, women, and adolescents. Eur J Public Health 14: 76–78.
- Jafarabadi MA, Allahverdipour H, Bashirian S, Jannati A (2012) Modeling the Underlying Predicting Factors of Tobacco Smoking among Adolescents. Iranian J Public Health 41: 46-57.
- Ahmadi J, Hasani M (2003) Prevalence of substance use among Iranian high school students. Addict Behav 28: 375-379.
- Serhier Z, Bennani Othmani M, Housbane S, Lembachar I, Moumaris M (2012) Smoking in public middle schools in Casablanca. Sante Publique24: 219-228.
- Xiao L, Jiang Y, Li Q, Feng GZ, Nan Y (2012) Study on the status of cigarette smoking in youths from three cities of China. Zhonghua Liu Xing Bing Xue Za Zhi 33: 676-680.
- Deesawat C, Boonshuyar C, Chansatitporn N, Viwatwonghasem C, Termsirikulchai L (2012) A multilevel study of smoking among youths in school at Buriram Province. J Med Assoc Thai95: S78-86.
- Roohafza H, Sadeghi M, Shahnam M, Bahonar A, Sarafzadegan N (2011) Perceived factors related to cigarette and waterpipe (ghelyan) initiation and maintenance in university students of Iran. Int J Public Health56: 175-180.
- Bonet de Luna C, López Giménez R (1993) Alcohol and tobacco consumption of middle school students in the municipality of Madrid [Article in Spanish]. An Esp Pediatr 38: 49-53.
- El Mhamdi S, Wolfcarius-Khiari G, Mhalla S, Ben Salem K, Soltani SM (2011) Prevalence and predictors of smoking among adolescent schoolchildren in Monastir, Tunisia. East Mediterr Health J 17: 523-528.
- Gaeta G, Del Castello E, Cuomo S, Effuso L, Pirera M, et al. (1998) Personal, familial and environmental factors influencing the inclination of smoking in adolescents: differences between sexes and between city and small-town dwellers (Article in Italian). Cardiologia 43: 417-426.
- Slama K, David-Tchouda S, Plassart JM (2009) Tobacco consumption among young adults in the two French departments of Savoie in 2008 [Article in French]. Rev Epidemiol Sante Publique 57: 299-304.
- Valdivia G, Simonetti F, Cumsille P, Ramírez V, Hidalgo CG, et al. (2004) Smoking habit in school age children, in Chile (Article in Spanish). Rev Med Chil 132: 171-182.
- Yang G, Ma J, Chen AP, Brown S, Taylor CE, et al. (2004) Smoking among adolescents in China: 1998 survey findings. Int J Epidemiol 33: 1103-1110.
- Hill D, Willcox S, Gardner G, Houston J (1987) Tobacco and alcohol use among Australian secondary school children. Med J Aust 146: 126-130.
- Hearn MD, Prokhorov AV, Murray DM, Alexandrov AA, Luepker RV (1991) Comparison of smoking prevalence in school students sampled from the United States of America and the Union of Soviet Socialist Republics. Int J Epidemiol 20: 413-415.
- Byckling T, Sauri T (1985) Smoking behavior and its determinants in 12-18 year old subjects. Acta Pediatr Scand Suppl 318: 195-203.
- Ogawa H, Tominaga S, Gellert G, Aoki K (1988) Smoking among junior high school students in Nagoya, Japan. Int J Epidermal 17: 814-820.
- al-Faris EA (1995) Smoking habits of secondary school boys in rural Riyadh. Public Health 109: 47-55.
- Whitehead M, Townsend P, Whitehead M, Davidson N (1992) Inequalities in health. London: Penguin 274-281.
- Leatherdale ST, Brown KS, Cameron R, McDonald PW (2005) Social modeling in the school environment, student characteristics, and smoking susceptibility: A multi-level analysis. J Adolesc Health 37: 330-336.
- Pierce JP (1989) International comparisons of trends in cigarette smoking prevalence. Am J Public Health 79: 152-157.
- Cavelaars AE, Kunst AE, Geurts JJ, Crialesi R, Grötvedt L, et al. (2000) Educational differences in smoking: international comparison. BMJ 320: 1102-1107.
- Nelson DE, Emont SL, Brackbill RM, Cameron LL, Peddicord J, et al. (1994) Cigarette smoking prevalence by occupation in the United States. A comparison between 1978 to 1980 and 1987 to 1990-1991. J Occup Med 36: 516-525.
- Pierce JP, Fiore MC, Novotny TE, Hatziandreu EJ, Davis RM (1992) Trends in cigarette smoking in the United States. Educational differences are increasing. JAMA 261: 56-60.
- Iribarren C, Luepker RV, McGovern PG, Arnett DK, Blackburn H (1997) Twelve-year trends in cardiovascular disease risk factors in the Minnesota heart study. Arch Intern Med 157: 873-881.
- Department of Tobacco Control (2001) Annual report on tobacco smoking. Isfahan Cardiovascular Research Center, Isfahan University of Medical Sciences (Iran).
- Song YM, Byeon JJ (2000) Excess mortality from avoidable and non-avoidable causes in men of low socioeconomic status: a prospective study in Korea. J Epidemiol Commun Health 54: 166-172.
- Anda RF, Williamson DF, Escobedo LG, Mast EE, Giovino GA, et al. (1990) Depression and the dynamics of smoking. JAMA 264: 1541-1545.
- Covey LS, Glassman AH, Stetner F (1990) Depression and depressive symptoms in smoking cessation. Compr Psychiatry 31: 350-354.
- Hall SM, Munoz R, Reus V (1991) Smoking cessation, depression and dysphoria. NIDA Res Monogr 105: 312-313.
- Dierker LC, Avenevoli S, Stolar M, Merikangas KR (2002) Smoking and Depression: An Examination of Mechanisms of Comorbidity. Am J Psychiatry 159: 947-953.
- Kendler KS, Neale MC, MacLean CJ, Heath AC, Eaves LJ, et al. (1993) Smoking and major depression: a causal analysis. Arch Gen Psychiatry 50: 36-43.
- Breslau N (1995) Psychiatric comorbidity of smoking and nicotine dependence. Behav Genet 25: 95-101.
- Windle M, Windle RC (2001) Depressive Symptoms and Cigarette Smoking Among Middle Adolescents: Prospective Associations and Intrapersonal and Interpersonal Influences. J Consult Clin Psychol 69: 215-226.
- Strine TW, Mokdad AH, Balluz LS, Gonzalez O, Crider R, et al. (2008) Depression and Anxiety in the United States: Findings From the 2006 Behavioral Risk Factor Surveillance System. Psychiatr Serv 59: 1383-1390.
- Rojas G, Gaete J, Guajardo V, Martínez V, Barroilhet S, et al. (2012) Association between drug consumption and depression among high school students. [Article in Spanish]. Rev Med Chil 140: 184-191.
- Carton S, Jouvent R, Widlöcher D (1994) Nicotine Dependence and Motives for Smoking in Depression. J Subst Abuse 6: 67-76.
- Mykletun A, Overland S, Aarø LE, Liabø HM, Stewart R (2008) Smoking in relation to anxiety and depression: Evidence from a large population survey: The HUNT study. Eur Psychiatry 23: 77-84.
- Johnson JG, Cohen P, Pine DS, Klein DF, Kasen S, et al. (2000) Association between cigarette smoking and anxiety disorders during adolescence and early adulthood. JAMA 284: 2348-2351.
- Koenen KC, Hitsman B, Lyons MJ, Niaura R, McCaffery J, et al. (2005). A twin registry study of the relationship between posttraumatic stress disorder and nicotine dependence in men. Arch Gen Psychiatry 62: 1258-1265.
- McCabe RE, Chudzik SM, Antony MM, Young L, Swinson RP, et al. (2004) Smoking behaviors across anxiety disorders. J Anxiety Disord 18: 7-18.
- Morissette SB, Tull MT, Gulliver SB, Kamholz BW, Zimering RT (2007) Anxiety, anxiety disorders, tobacco use, and nicotine: a critical review of interrelationships. Psychol Bull 133: 245-272.
- DeHaas RA, Calamari JE, Bair JP, Martin ED (2001) Anxiety sensitivity and drug or alcohol use in individuals with anxiety and substance use disorders. Addict Behav 26: 787-801.
- Bernstein GA, Borchardt CM (1991) Anxiety disorders of childhood and adolescence: A critical review. J Am Acad Child Adolesc Psychiatry 30: 519-532.
- Boyd CP, Kostanski M, Gullone E, Ollendick TH, Shek DT (2000) Prevalence of anxiety and depression in Australian adolescents: Comparisons with worldwide data. J Genet Psychol 161: 479-492.
- Tomb M, Hunter L (2004) Prevention of anxiety in children and adolescents in a school setting: The role of school-based practitioners. Children & School 26: 87-101.
- Tramonte L, Willms D (2010) The Prevalence of Anxiety Among Middle and Secondary School Students in Canada. Can J Public Health 101: S19-S22.
- Patton GC, Hibbert M, Rosier MJ, Carlin JB, Caust J, et al. (1996) Is Smoking Associated with Depression and Anxiety in Teenagers? Am J Public Health 86: 225-230.
- Petersen AC, Compas BE, Brooks-Gunn J, Stemmler M, Ey S, et al. (1993) Depression in adolescence. Am Psychol 48: 155-168.
- Malkin SA, Allen DL (1980) Differential characteristics of adolescent smokers and nonsmokers. J Fam Pract 10: 437-440.
- Deb S, Chatterjee P, Walsh K (2010) Anxiety among high school students in India: Comparisons across gender, school type, social strata and perceptions of quality time with parents. AustJ Edu DevelopPsychol 10: 18-31.
- Brown RA, Lewinsohn PM, Seeley JR, Wagner EF (1996) Cigarette smoking, major depression, and other psychiatric disorders among adolescents. J Am Acad Child Adolesc Psychiatry 35: 1602-1610.
- Costello EJ, Erkanli A, Federman E, Angold A (1999) Development of psychiatric comorbidity with substance abuse in adolescents: Effects of timing and sex. J Clin Child Psychol 28: 298-311.
- Grant BF, Hasin DS, Chou SP, Stinson FS, Dawson DA (2004) Nicotine dependence and psychiatric disorders in the United States: Results from the National Epidemiologic Survey on Alcohol and Related Conditions. Arch Gen Psychiatry 61: 1107-1115.
- Mitchell RE, Matthews JR, Grandy TG, Lupo JV (1983) The question of stress among first year medical students. J Med Edu 58: 367-372.
- Covey LS, Tam D (1990) Depressive mood, the single-parent home, and adolescent cigarette smoking. Am J Public Health 80: 1330-1133.
- Waal-Manning HJ, de Hamel FA (1978) Smoking habits and psychometric scores: a community study. N Z Med J 88: 188-191.
- Mehrabian A (2001) General Relations among Drug Use, Alcohol Use, and Major Indices of Psychopathology. J Psychol 135: 71-86.
- Cherry N, Keirnan KE (1978) A longitudinal study of smoking and personality. In: Thornton RE, ed. Smoking Behaviour: Physiological and Psychological Influences. New York, NY: Churchill Livingston.
- Breslau N, Kilbey MM, Andreski P (1993) Nicotine dependence and major depression: new evidence from a prospective investigation. Arch Gen Psychiatry 50: 31-35.
- Penny GN, Robinson JO (1986) Psychological resources and cigarette smoking in adolescents. Br J Psychol 77: 351-357.
- Mykletun A, Stordal E, Dahl AA (2001) Hospital anxiety and depression (HAD) scale: factor structure, item analyses and internal consistency in a large population. Br J Psychiatry179: 540-544.
- Breslau N, Peterson EL (1996) Smoking cessation in young adults: age at initiation of cigarette smoking and other suspected influences. Am J Publ Health 86: 214-220.
- Botvin GJ (2000) Preventing drug abuse in schools: social and competence enhancement approaches targeting individual-level etiologic factors. Addict Behav 25: 887-897.
- Hawkins JD, Catalano RF, Miller JY (1992) Risk and protective factors for alcohol and other drug problems in adolescence and early adulthood: Implications for substance abuse prevention. Psychol Bull 112: 64-105.
- Sawadi H (1999) Individual risk factors for adolescence substance use. Drug Alcohol Depen 55: 209-224.
- Centers for Disease Control and Prevention (CDC) (2011) Smoking in Top-Grossing Movies, United States, 2010. MMWR Morb Mortal Wkly Rep 60: 909-1003.