Case Report
Mehdi Soufi*1, Ahmed Mimouni2, Ghizlane Kharrasse3, EL Harroudi Tijani1, and Mohammed Bouziane1
1Department of Digestive Surgery, Faculty of medicine Oujda, University Mohammed first, Oujda -Morocco
2Department of Genecology, Faculty of medicine Oujda, University Mohammed first, Oujda -Morocco
3Department of Gastroenterology, Faculty of medicine Oujda, University Mohammed first, Oujda -Morocco
Corresponding author
Mehdi Soufi, MD, Division of digestive Surgery, Oujda CHU, Faculty of medicine. University Mohammed first, Bp 4847 Oujda university 60049, oujda Morocco, Tel: +212661212924; E-mail: drsoufimehdi@hotmail.fr
Received Date: 29thSeptember 2014
Accepted Date: 27th January 2015
Published Date: 05th February 2015
Citation
Soufi M, Mimouni A, Kharrasse G, Tijani el H, Mohammed B (2015) Intestinal Endometriosis Revealed by a Ileocolic Intussusception. Enliven: Gynecol Obstet 1(1):006
Copyright
@ 2015 Dr. Mehdi Soufi. This is an Open Access article published and distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Intestinal endometriosis is very rarely manifested by an acute bowel obstruction secondary to ileo-cecal intussusception. We report a case of a 47-year-old female patient with symptoms and signs of an acute small bowel obstruction. CT scan confirmed the intussusception. A right colectomy for suspected malignancy was performed with an ileocolic anastomosis. Histological examination revealed an endometriosis of the ileocecal junction.
Introduction
First described by Sabiard in 1696, endometriosis is an estrogen-dependent inflammatory disease characterised by the presence of endometrial tissue outside the uterine cavity [1-4]. It has been more likely described in pelvic organs but also has been described in several sites of the body (omentum, gastrointestinal tract (rectosigmoid, appendix, small bowel, right colon), umbilicus, lungs, kidney, pancreas and liver) [2-4]. We report a rare case of a woman who presented an ileocecal intussusception due to ileocecalendometriosis.
Observation
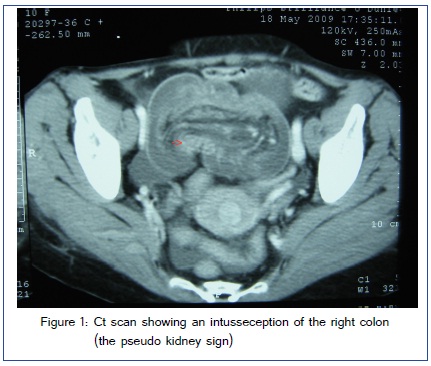
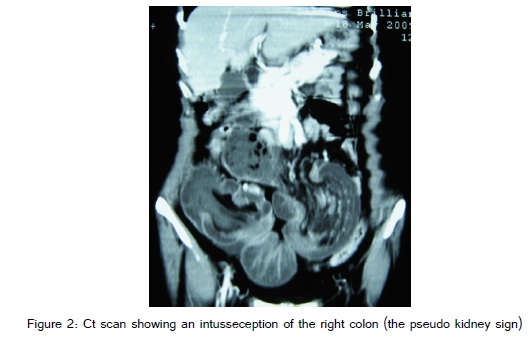
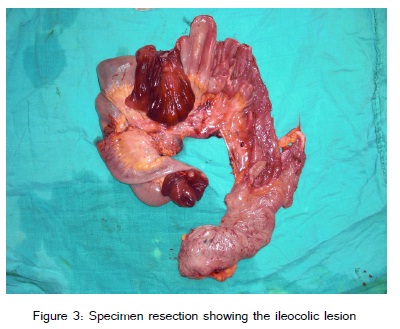
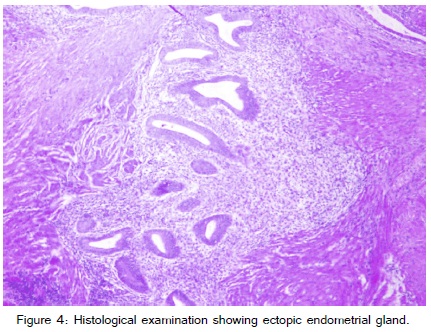
A 47-year-old G0P0 Moroccan woman admitted to emergency department for an acute abdominal pain accompanied with vomiting and rectal bleeding evolving for 24 hours. She didn?t have any medical or surgical history such as dysmenorrhea, dyspareunia, non-menstrual abdominal pain, dyschezia, or intestinal complains, the physical exam noted a right fossa palpable mass, painful without lymphadenopathy. Complete blood count test revealed an anemia with a Hemoglobin level at 7.0 g/dL and a leucocytosis with a White Blood Cell Count of 14,000/mm3. The computed tomography scan showed a pseudo kidney image at the right colon level (figure 1 and figure 2). The preoperative suspected diagnosis was a colon caecum tumor (malignant or benign). An exploratory laparotomy was performed and revealed an irreducible ileocolic intussusception. No other lesion of endometriosis has been detected. A right hemicolectomy with ileocolic an astomosis was performed (figure 3). Macroscopically, an ileal solid tumor of 2x3cm large was intussuscepted into the right colon. Histopathological examination revealed the presence of intestinal endometriosis of the ileocolic segment (figure 4). The postoperative course was uneventful. The patient was discharged on the fifth postoperative day and was referred in parallel to a gynaecologist for management of her endometriosis.
Discussion
Intussusception, known as the invagination of a segment of the gastrointestinal tractinto an immediately adjacent portion, is a rare condition in the adult population accounting for less than 5% of all intussusceptions [4]. It affects mainly the small intestine (52%?55%), while the colon is affected in 38%?45% of cases. Various methods have been applied in the classification of intussusception [5]. Based on location, it has been classified into four categories: enteroenteric, colocolic, ileocolic, and ileo-cecal. Ileocolic intussusceptions are defined as those with prolapse of the ileum through the ileo-cecal valve into the colon and they constitute 15% of all intussusceptions [6]. In contrast with the primitive forms of infants, an organic lesion is found in 80% of cases in adults, usually benign in the small intestine and malignant in the colon [7].
Clinical presentation of intussusception varies, and the symptoms are wide-ranging and often nonspecific. The signs and symptoms are often chronic, consistent with partial obstruction and not with an acute abdomen. Abdominal computed tomography (CT) is useful to confirm intussusception, as in our case, with a variable diagnostic accuracy (ranging from 58% to 100%) [8]. At CT, three different appearances for intussusception have been described, reflecting the severity and duration of the disease process. A target appearance is the earliest sign that progresses on to a sausage-shaped mass of different layers of attenuation, representing mesenteric fat and bowel wall, and finally, a reniform mass develops due to oedema, mural thickening and vascular compromise [9]. Recently, multi-detector computerized tomography enteroclysis has been suggested for the diagnosis of bowel endometriosis with good sensitivity, this examination need a bowel preparation and therefore difficult to practice in emergency.
Endometriosis is now recognized in up to 20% of menstruating women [3]. Intestinal localization have been reported with the rectosigmoid colon, small bowel, appendix and caecum affected respectively in 50-90%, 2-16%, 3-18% and 2-5% of cases [2,10]. Ileocecal incidence involvement is rare (about 3%) [11]. The aetiology of endometriosis remains unknown [12]. Many theories have been proposed to explain this disease and the most accepted is that of « retrograde menstruation » causing implantation and growth of endometriosis on the serosal surface of extra-uterine organs or occurring secondary to metaplasia in the pelvic peritoneum [13].
Endometriosis is a rare cause of intestinal intussusception. The pathophysiology of the symptoms varies with the topography of the lesions. Serous lesions cause contractures and peritoneal adhesions with intestinal fibrosis while the mucosa and muscularis mucosa damage induce a reactive smooth muscle hyperplasia creating intraluminal pseudotumors. These lesions cause a peristaltic hyperactivity and a peristaltic asynchronism, favouring invaginations [14]. In our patient, intussusception was evolving insidiously and was declared in an acute way by a bowel obstruction syndrome.
Intestinal endometriosis is a challenging condition to diagnose as it can manifest with acute and chronic symptoms that can mimic many different benign and malignant pathologies [2,14]. The case presented is rarely seen, as small bowel obstruction only accounts for less than 1% of all surgical resections for endometriosis [15,16]. Moreover, rectal bleeding, as it was diagnosed in our patients is an uncommon symptom in intestinal involvement and it can strongly mimic a colorectal cancer [15].
Microscopic evaluation of the intussusceptum is the only examination that will confirm the diagnosis of endometriosis [3]. However, MRI has an excellent sensitivity for detecting enteric endometriosis but distinguishing between serous and deep lesions can be difficult in MRI, which may also miss sigmoid, caecal/appendicular or small intestine lesions [17]. The treatment of intussusception caused by ileal endometriosis consists of surgical resection of the affected intestinal part with termino-terminal anastomosis, as was the case of our patient. Surgery is strongly advised when it is impossible to exclude a malignancy [6,18]. If the endometriosis is suspected intra operatively, then as many ectopic lesions as possible should be excised [1,19]. Small bowel endometriosis tends to only affect the bowel serosa and deposits tend not to be greater than 2cm in size; therefore, a resection margin of greater than 2cm should be attempted [14]. Some authors suggest a post-operative hormonal therapy; yet it is failed to demonstrate any benefits in the literature [20].
Conclusion
Intussusception is a rare cause of bowel obstruction affecting adults, and endometriosis as its underlying lesion is even less common. This case highlights the difficulty of preoperative diagnosis. Thus, intestinal endometriosis should be considered in the differential diagnosis in a reproductive age women who presents with bowel obstruction symptoms.
References
2. Giudice LC, Kao LC (2004) Endometriosis. Lancet 364: 1789-1799.
18. Azar T, Berger DL (1997) Adult intussusception. Ann Surg 226: 134-138.