Original Article
Zhi-Hong Zhao1*, Hua He2, Jun Luo1, Wei-jian Jiang1, Chan Jin1, Jun Chen1, Sai-hua Wang1, Zhong-ping Ning1, Chang-zhu Zheng1, Pei Tian1, Dan-jie Lu1, and Xin-ming Li1*
1Department of Cardiology of the ZhouPu Hospital, Pudong District, Shang Hai,201318, P.R. China
2Department of Emergency Cardiology, Beijing Anzhen Hospital, Capital Medical University, Beijing 100029, P.R, China
Corresponding author
Dr. Zhi-Hong Zhao, Department of Cardiology of the ZhouPu Hospital, Pudong District, 201318, P.R. ShangHai, China; Tel: +86 210 68135590 ext. 3122; E-mail: zhihong_zhao@126.com
Dr. Xin-ming Li, Department of Cardiology of the ZhouPu Hospital, Pudong District, 201318, P.R. ShangHai, China; Tel: +86 210 68135590 ext. 3122; E-mail: xinmingli6@126.com
Received Date: 16th March 2015
Accepted Date: 10th April 2015
Published Date: 16th April 2015
Citation
Zhao ZH, He H, Luo J, Jiang WJ, Jin C, Chen J, Wang SH, Ning ZP, Zheng CZ, Tian P, Lu DJ, and Li XM (2015) Fibroatheroma Morphological Features of Borderline Coronary Lesion Plaques on Stable Angina Pectoris Patients. Enliven: Clin Cardiol Res 2(1): 002.
Copyright
@ 2015 Dr. Zhi-Hong Zhao and Xin-ming Li. This is an Open Access article published and distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
The aim of this study is to investigate the lesion-related specific morphological characteristics of borderline coronary lesion plaques which are responsible for stable angina pectoris. 86 borderline coronary lesion plaques from stable angina pectoris patients were analyzed by using virtual histology-intravascular ultrasound (VH-IVUS). Patients’ characteristics were compared. In the laboratory findings, coronary artery disease distribution and virtual histologyintravascular ultrasound detected thin-cap fibroatheroma (TCFA) and thick-cap fibroatheroma (ThCFA) phenotype groups which were tested. Analysis of the borderline coronary lesion plaques indicate major ratio of fibroatheroma, pathological intimal thickening, and less fibrotic plaque. TCFA and ThCFA accounts for only 25% and 33% of the plaque lesions. Fibrofatty and dense calcium tissues improved in TCFA group (P<0.05), and VH-TCFA III, IV account for 45.9%, 43.3% repressively in subtypes. These findings suggest that for angina pectoris with borderline coronary lesion plaques, TCFA occupied only 1/4 proportion of the plaque lesions and the clinical characteristics were similar to ThCFA patients, which may be responsible for the cardiovascular events.
Keywords
Angina pectoris; Borderline coronary lesion; Virtual histology-intravascular ultrasound; Thin-cap fibroatheroma; Thick-cap fibroatheroma
Introduction
Despite the advances in medical interventional and surgical therapies for the atherosclerosis coronary disease, this disease still remains the principal killer in both western and the developing countries [1], and better understanding of atherosclerosis is therefore needed in order to prevent its devastating effects worldwide.
Atherosclerotic plaque rupture and thrombosis is the main cause for the majority of acute coronary syndromes (ACS) and sudden coronary death. The precursor lesion of plaque rupture is a thin cap fibroatheroma or ?vulnerable plaque?. Erosion and calcified nodule are two other mechanisms for the presence of luminal thrombosis. The in vivo histological characterization of coronary plaques using VH-IVUS has been successfully validated [2].VH-IVUS was used to assess no culprit lesions in patients with acute coronary syndrome demonstrating the predictive value, albeit modest, with virtual histology of TCFA. However, in vivo VH-IVUS studies of culprit lesions have included few patients and the results have contradicted each other and also contradicted findings from histopathological studies. It is clinically significant to more accurately define the characteristics of vulnerable plaque [3]. Here, we designed a prospective VH-IVUS study to assess the characteristics of borderline coronary lesion (BCL) plaques on patients with angina pectoris and to determine the characteristic histological profile of atherosclerosis plaque of fibroatheroma, including TCFA and ThCFA.
Methods
Study Population
Consecutive patients who underwent IVUS examinations of stable angina pectoris with BCL arteries between January 2014 and October 2014 were included in the analysis. IVUS images were digitally recorded and analyzed by ZhouPu Hospital cardiovascular laboratory. Patients presenting to the cardiac catheterization laboratory at ZhouPu Hospital with chest pain, abnormal non-invasive stress test, stable angina syndromes and non-obstructive cardiovascular lesion found by computed tomographic angiography were enrolled. Unstable angina and ACS patients were excluded in the cases such as suboptimal IVUS image quality, unsuccessful IVUS pullbacks, and no clearly identified lesion by VH-IVUS. Finally, 86 patients were included in this study. This study protocol was approved by the Ethics Committee of the ZhouPu Hospital. All patients signed informed written consent.
Laboratory Tests
Venous blood samples were collected within 6-12 hours of admission. Six milliliter plasma samples were collected using ethylene diamine tetra acetic acid as an anticoagulant. Fasting blood samples were analyzed for total cholesterol (CHOL), low density lipoprotein cholesterol (LDL-C), high density lipoprotein cholesterol (HDL-C), and triglycerides (TG) in a routine diagnostic analyzer using enzymatic colorimetric assays. NT-ProBNP, GLU and GlcHb were measured too. All of which were measured by an automated immunoassay analyzers (ARCHITECT ci16200 Integrated System, Abbott).
Acquisition of IVUS Images
All patients underwent coronary angiography. An IVUS catheter was inserted into the coronary artery through a 6-F coronary guiding catheter over a 0.014-inch guidewire. Three-vessel gray-scale intracoronary imaging of the left main and proximal 6 to 8 cm of each of the major epicardial coronary arteries was performed with the use of a synthetic aperture-array, 20-MHz, 3.2-French catheter (phased-array 20 MHz Eagle Eye® Gold Catheter and Volcano S5i® Imaging System (Volcano Corporation, Rancho Cordova, California). VH-IVUS imaging was performed by locating the IVUS catheter in the coronary artery using a fiduciary side branch as the starting point and using an automated continuous pullback at a rate of 1 mm/s (R-100 Imaging Catheter Pullback Device, Volcano Corporation, Rancho Cordova, California) after administration of systemic heparin 6000U and 200 ?g of intracoronary nitroglycerine. The data were analyzed by using echoPlaque4 software (INDEC Systems, Inc. Santa Clara, CA). The plaque burden was defined as plaque and media cross-sectional area divided by an external elastic membrane cross-sectional area.
The BCL plaques was defined as a segment with a plaque burden of ?40% but ?70% in three consecutive slices (1.5 mm in length) [4,5]. The regions of interested and analysis were defined in lesion vessel as the lesion plus 5 VH-IVUS frame of proximal and distal to the edges of the narrowest lesion, with the following exception. VH-IVUS plaque components were color coded as dense calcium, necrotic core, fibrofatty, or fibrotic. Lesions were further classified by means of VH-IVUS as one of the following: TCFA, ThCFA, pathological intimal thickening (PIT), fibrotic plaque (FT), or fibrocalcific plaque (FC) (Figure1). Fibroatheroma was defined as >10% confluent necrotic core, and TCFA as fibroatheroma with necrotic core in direct contact with the lumen in at least 3 consecutive VH-IVUS frames. ThCFA was a fibroatheroma with a definable fibrous cap. PIT had a mixture of all plaque components, but dominantly fibrofatty plaque with <10% confluent necrotic core and <10% confluent dense calcium. FT had mainly fibrotic with <10% confluent necrotic core, <10% confluent dense calcium, and <15% fibrofatty plaque. FC had mainly fibrotic with >10% confluent dense calcium, but <10% confluent necrotic core. All of the above-mentioned criteria should be present in three consecutive frames for a lesion to be considered of a particular category. TCFA lesions with a plaque burden of at least 70% were classified as large TCFA lesions [6-9].

Figure 1. Classification of plaque morphology with intravascular ultrasound virtual histology. TCFA, thin-cap fibroatheroma; ThCFA, thick-cap fibroatheroma; PIT, pathological intimal thickening; FT, fibrotic plaque; FC, fibrocalcific plaque[9].
VH-TCFA were Classified as the Following [10]
VH-TCFA I, less than 5% calcium; VH-TCFA II, more than 5% calcium; VH-TCFA III, multiple strata; VH-TCFA IV, necrotic core greater than 20%, calcium more than 5%, remodeling greater than 1.05, and plaque burden greater than 50%. These criteria must be met on three consecutive frames. We selected a plaque burden >50% but <70% to be combined with plaque phenotype for our investigation of plaque vulnerability.
Statistical Analysis
Statistical analysis was performed with IBM SPASS Statistics software, version 19 (company, location). Categorical variables were summarized using counts and percentages. Continuous variables for baseline clinical characteristics were displayed as median, first and third interquartile range. For lesion level data, a model with a generalized estimating equation approach was used to compensate for any potential cluster effect of multiple lesions in the same patient and presented as least square means with 95% confidence intervals. A P value <0.05 was considered to indicate statistical significance.
Results
Clinical Characteristics of the Study Population
The basic characteristics of the BCL groups are outlined in (Table 1). There were no statistically significant differences in patient characteristics, including age, sex, smoking, diabetes mellitus, hypertension, and hyperlipidemia. The cardiac function, coronary artery disease distribution showed no statistically significant differences; There were no statistically significant differences in blood lipidemia, renal function, NT-ProBNP between the groups (P >0.05).
| TCFA Patients(n = 36) | ThCFA Patients(n = 50) | p Value | |
| Patient characteristics | |||
| Age, yrs | 66.97±9.72 | 66.18±9.6 | 0.234 |
| Male, n (%) | 14 (39) | 22 (44) | >0.05 |
| Smoking, n (%) | 7(19) | 13 (26) | >0.05 |
| Diabetes mellitus, n (%) | 10 (27) | 13 (26) | 0.03 |
| Hypertension, n (%) | 24 (68) | 39(78) | >0.05 |
| Hyperlipidemia, n (%) | 15 (41) | 19 (38) | >0.05 |
| Procedural characteristics | |||
| NYHA | |||
| ?-?,n(%) | 35(97.2) | 48(96) | 0.08 |
| ?-?,n(%) | 1(2.8) | 2(4) | 0.08 |
| Laboratory findings | |||
| APOA1 | 1.32±0.21 | 1.26±0.2 | 0.874 |
| APOB | 0.91±0.21 | 0.89±0.21 | 0.985 |
| CHOL | 4.53±1.00 | 4.08±1.48 | 0.202 |
| HDL-C | 1.15±0.22 | 4.54 ±21.01 | 0.509 |
| LDL-C | 2.73±0.92 | 2.52±0.9 | 0.126 |
| LPa | 197.65±103.32 | 166.29±95.72 | 0.56 |
| TG | 1.91±1.50 | 1.34±0.9 | 0.048 |
| BUN | 6.45±3.3 | 4.97±3.48 | 0.718 |
| CREA | 71.14±30.68 | 68.70 ±29.51 | 0.784 |
| UA | 334.2(211.3,530.59) | 318(268.6,411.5) | 0.132 |
| NT-ProBNP | 222.5(147,591) | 244(110,1009) | 0.122 |
| GLU | 5.88±1.13 | 5.65±2.53 | 0.018 |
| GlcHb | 5.30±2.01 | 5.50±2.56 | 0.092 |
| Coronary artery disease | |||
| LAD, n (%) | 18(50) | 29(58) | >0.05 |
| LCX, n (%) | 9(25) | 7(14) | >0.05 |
| RCA, n (%) | 9(25) | 14(28) | >0.05 |
| PCI performed, n (%) | 7(19.4) | 13(26) | >0.05 |
Table1. Patient characteristics in the entire cohort
Values are mean ± SD, n (%), or median (25th, 75th percentile). APOA1 = apolipoprotein A1; APOB= Apolipoproteins B; CHOL = cholesterol levels; HDL-C = high-density lipoprotein cholesterol; LDL-C = low-density lipoprotein cholesterol; TG = triglycerides; LPa =lipoprotein a; BUN= blood urea nitrogen; CREA= creatinine; UA= uric acid; NT-ProBNP= Brain Natriuretic Peptide; GLU= Glucose; GlcHb= glycated hemoglobin; TNI= troponin-I; CKMB= creatinine kinase, MB isoenzyme; MYO= myoglobin. LAD= left anterior descending; LCX= left circumflex; CA= right coronary artery.
IVUS Findings
Among patients, lesions were classified by VH-IVUS including: Fibroatheroma (TCFA, ThCFA), PIT, FT, and FC. IVUS findings are presented in (Table 2). Compared with TCFA Patients, plaque burden, plaque area, vessel area were greater in ThCFA Patients (P < 0.05). Fibrofatty and dense calcium tissues in TCFA patients were greater compared to ThCFA Patients. The ratio of fibroatheroma is 52% ( TCFA, 22%; ThCFA, 30% respectively); also the percentage of PIT, FT, FC were 28%, 2%, 18% respectively (Figure 2A).VH-TCFA were classified as the following (Figure 2B), the percentage of VH-TCFA III and VH-TCFA IV were 45.9%, 43.3% respectively.
| TCFA Patients (n =36) | ThCFA Patients (n =50) | p Value | |
| Lesion segment | |||
| Plaque burden, % | 60.16±12.23 | 64.59±8.06 | 0.048 |
| Plaque Area , mm2 | 8.98±3.77 | 11.02±3.62 | 0.013 |
| Vessel Area , mm2 | 14.71±5.03 | 16.86±4.18 | 0.034 |
| MLA , mm2 | 5.73±2.16 | 5.83±1.46 | 0.798 |
| MLA?4.0mm2 n (%) | 7?19? | 2?4? | >0.05 |
| FT area (%) | 58.19±8.93 | 59.59±10.23 | 0.603 |
| FF area (%) | 14.08±13.29 | 1.42±0.99 | 0.001 |
| NC area (%) | 21.73±10.91 | 19.28±8.38 | 0.242 |
| DC area (%) | 5.98±4.66 | 3.75±3.54 | 0.013 |
Table 2. IVUS Findings of the Fibroatheroma
Study participants and the presence of coronary lesions on intravascular ultrasound. VH-IVUS. Data are shown as mean ± SD and/or n (%); MLA, minimal luminal area; FT, fibrous tissue; FF, fibrofatty tissue; NC, necrotic core; DC, dense calcium; LA, minimal luminal area; TCFA, thin-cap fibroatheroma. ThCFA, thick-cap fibroatheroma.SD, standard deviation, A p value <0.05 was considered significant.
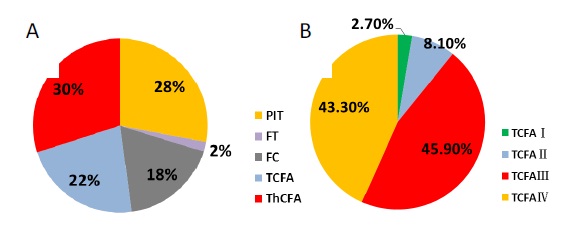
Figure 2A. Prevalence of virtual histology of four types of coronary artery plaque, TCFA, ThCFA, PIT, FT and FC. Figure 2B. corresponding subtypes of TCFA.
Discussion
The novel findings in the study were that the stable angina pectoris with BCL on angiography, compared to the VH-IVUS detected TCFA and ThCFA phenotype groups, the patient characteristics, laboratory findings, coronary artery disease distribution showed no difference. Among our research of BCL on stable angina pectoris, the ratio of fibroatheroma is major, the next is PIT and FT. TCFA and ThCFA takes only 1/4 and 1/3 proportion of the BCL plaque lesions, which means that few BCLs belonged to ?vulnerable plaque?. Also we found that fibrofatty tissue improved significantly in TCFA group, and VH-TCFA III, IV were the major types of subtypes, 45.9%, 43.3% repressively.
Atherosclerosis is a lipoprotein-driven disease that leads to plaque formation at specific sites of the arterial tree through intimal inflammation, necrosis, fibrosis, and calcification. Atherosclerosis causes clinical disease through luminal narrowing or by precipitating thrombi that obstruct blood flow to the coronary, caused stable angina pectoris and the acute coronary syndromes. In recent years, observations on the natural history of coronary plaque and newly available intravascular tools such as IVUS, virtual histology, palpography, and thermography fueled interest in the local plaque. Physicians emphasize on understanding, diagnosing, and treating atherosclerosis as a systemic disease and then took hold as medications, rather than locally targeted therapies, demonstrated efficacy in reducing myocardial infarction and death [11,12]. The shift was punctuated by results of the COURAGE trial in which an initial strategy of revascularization conferred no advantage for prevention of the composite of death or nonfatal myocardial infarction above and beyond optimal medical therapy [13]. Also research has shown that certain coronary plaque characteristics, especially the fibrous cap, inflammation, and the necrotic core size can predict the likelihood of future cardiovascular adverse events. Culprit lesions of patients, who have had an ACS commonly, are ruptured coronary plaques with superimposed thrombus, the precursor of such lesions is an inflamed TCFA [14].
Assessment of a coronary lesion with intermediate severity that continues is a challenge for cardiologists [5]. Atherosclerotic plaque rupture with luminal thrombosis is the most common mechanism responsible for the majority of ACS and sudden coronary death. The precursor lesion of plaque rupture is thought to be a TCFA or ?vulnerable plaque?. The rupture of fibrous caps occurs at their weakest points, e.g.: near shoulder regions, at the mid portion of the fibrous cap. Once the fibrous cap ruptures, the necrotic core contents are exposed to the circulating blood, coagulation cascade involving platelets is activated in response to the exposure of lipids and tissue factors which are present in the necrotic core [15,16]. Notwithstanding there have some adverse views, for example, VH-IVUS study showed the absence of TCFA in up to 50% of ACS patients [17], the fissure of TCFA may not necessarily lead to ACS where asymptomatic plaque fissure is a frequent event leading to plaque progression [18], Yonetsu et al found that about 15% of patients with stable angina presented plaque fissure using optical coherence tomography [19], suggesting heterogeneity in culprit plaque composition leading to coronary instability. The reasons why some plaque fissures lead to ACS while others do not, is still kept unknown. Finally, it is worth noting that coronary instability is associated with systemic evidence of inflammation in 50% of patients only [20].
There are series studies on the plaque characteristics of ACS and Acute myocardial infarction with ST elevation. VH-IVUS were used to investigate the factors which influence blood flow restoration after thrombolysis. The results show that the NC content of atherosclerotic plaques is significant for flow restoration after the occurrence of a coronary event [21]. CULPLAC study showed that the presence of VH-TCFAs, calcified nodules, positive remodeling, and a high necrotic core volume are associated with a culprit plaque [10]. Another study on VH of atherosclerotic plaque composition in patients with stable angina and ACS showed that the VH-IVUS detected-necrotic core was significantly larger in atherosclerotic lesions in patients in ACS compared to the stable angina subjects. It could be used as a marker of plaque vulnerability [22]. PROSPECT study showed that the prevalence of secondary, during 3 years of follow-up, 14.1% of patients with ACS had no culprit plaque ruptures were associated with a VH fibroatheroma phenotype with a residual necrotic core in three-fourths of patients and a VH-TCFA phenotype with a residual necrotic core in approximately one-half of patients, and that it was not associated with subsequent major adverse cardiovascular events in patients treated with proper medical therapy [23]. This means that the TCFA of the BCL perhaps risk factors.
Our study is based on the clarification of the plaque characteristics of stable angina pectoris with BCL on angiography, We illustrated the relationship between TCFA and ThCFA phenotype. Our research found that TCFA occupied only 1/4 proportions of the BCL plaque lesions, except that the fibrofatty tissue component augmented markedly, other clinical and IVUS characteristics analogously to the ThCFA group. Among TCFA patients, the largest proportion of TCFA III, IV is 89.2%. Marzilli et al. [24] pointed out that coronary artery obstruction is only 1 element in a complex multifactorial pathophysiological process that leads to ischemic heart disease and that the presence of obstructive lesions in patients with ischemic heart disease does not necessarily imply a causative role. The myocardial cell should be put at the center of the model. The potential pathological inputs that might drive progression to unstable angina, acute myocardial infarction, and sudden cardiac death can be considered, starting with obstructive atherosclerosis but also including inflammation, endothelial dysfunction, microvascular dysfunction, platelet dysfunction, thrombosis, and vasomotor dysfunction. From above researches, we can see that coronary plaque property is the major substrate, notwithstanding the BCLs, only a trifle of percentage, should be oriented. We thought that these categories of patients, coronary intervention therapy should be fully considered.
Study Limitations
The authors only observed the morphological characteristics of the BCL plaques of the angina pectoris, and not consider the therapy therapeutic schedule. The patients should be followed-up, and should be observed for the major adverse cardiac events with different treatment strategies, e.g. intensive medication or early PCI. Because of a relatively small number of patients included in our study both ostial and bifurcation lesions were not examined. The decision to perform pre-intervention IVUS was at the discretion of the operator, potentially lead to a selection bias.
Conclusion
These findings suggest that for angina pectoris with BCL plaques, TCFA takes only 1/4 proportion of the plaque lesions, which may be responsible for the cardiovascular events.
Conflict of Interest
None.
Acknowledgement
Financial support from the Zhou Pu Hospital Medical Foundations.
References
- Taqueti VR, Hachamovitch R, Murthy VL, Naya M, Foster CR, et al. (2015) Global coronary flow reserve is associated with adverse cardiovascular events independently of luminal angiographic severity and modifies the effect of early revascularization. Circulation 131: 19-27.
- Wu X, Maehara A, Mintz GS, Kubo T, Xu K, et al. (2010) Virtual histology intravascular ultrasound analysis of non-culprit attenuated plaques detected by grayscale intravascular ultrasound in patients with acute coronary syndromes. Am J Cardiol 105: 48-53.
- Amano H, Wagatsuma K, Yamazaki J, Ikeda T (2013) Virtual histology intravascular ultrasound analysis of attenuated plaque and ulcerated plaque detected by gray scale intravascular ultrasound and the relation between the plaque composition and slow flow/no reflow phenomenon during percutaneous coronary intervention. J Interv Cardiol 26: 295-301.
- Gogas BD, Farooq V, Serruys PW, Garcia-Garcia HM (2011) Assessment of coronary atherosclerosis by IVUS and IVUS-based imaging modalities: progression and regression studies, tissue composition and beyond. Int J Cardiovasc Imaging 27: 225-237.
- Tobis J, Azarbal B, Slavin L (2007) Assessment of intermediate severity coronary lesions in the catheterization laboratory. J Am Coll Cardiol 49: 839-848.
- Garcia-Garcia HM, Mintz GS, Lerman A, Vince DG, Margolis MP, et al. (2009) Tissue characterisation using intravascular radiofrequency data analysis: recommendations for acquisition, analysis, interpretation and reporting. EuroIntervention 5: 177-189.
- Kubo T, Maehara A, Mintz GS, Doi H, Tsujita K, et al. (2010) The dynamic nature of coronary artery lesion morphology assessed by serial virtual histology intravascular ultrasound tissue characterization. J Am Coll Cardiol 55: 1590-1597.
- Corban MT, Eshtehardi P, Suo J, McDaniel MC, Timmins LH, et al. (2014) Combination of plaque burden, wall shear stress, and plaque phenotype has incremental value for prediction of coronary atherosclerotic plaque progression and vulnerability. Atherosclerosis 232: 271-276.
- Nair A, Margolis MP, Kuban BD, Vince DG (2007) Automated coronary plaque characterisation with intravascular ultrasound backscatter: ex vivo validation. EuroIntervention 3: 113-120.
- Cascon-Perez JD, de la Torre-Hernandez JM, Ruiz-Abellon MC, Martinez-Pascual M, Marmol-Lozano R, et al. (2013) Characteristics of culprit atheromatous plaques obtained in vivo by intravascular ultrasound radiofrequency analysis: results from the CULPLAC study. Am Heart J 165: 400-407.
- Tomey MI, Narula J, Kovacic JC (2014) Advances in the understanding of plaque composition and treatment options: year in review. J Am Coll Cardiol 63: 1604-1616.
- Niccoli G, Liuzzo G, Montone RA, Crea F (2014) Advances in mechanisms, imaging and management of the unstable plaque. Atherosclerosis 233: 467-477.
- Boden WE, O'Rourke RA, Teo KK, Hartigan PM, Maron DJ, et al. (2007) Optimal medical therapy with or without PCI for stable coronary disease. N Engl J Med 356: 1503-1516.
- Garcia-Garcia HM, Jang IK, Serruys PW, Kovacic JC, Narula J, et al. (2014) Imaging plaques to predict and better manage patients with acute coronary events. Circ Res 114: 1904-1917.
- Sakakura K, Nakano M, Otsuka F, Ladich E, Kolodgie FD, et al. (2013) Pathophysiology of atherosclerosis plaque progression. Heart Lung Circ 22: 399-411.
- Bentzon JF, Otsuka F, Virmani R, Falk E (2014) Mechanisms of plaque formation and rupture. Circ Res 114: 1852-1866.
- Fujii K, Kobayashi Y, Mintz GS, Takebayashi H, Dangas G, et al. (2003) Intravascular ultrasound assessment of ulcerated ruptured plaques: a comparison of culprit and nonculprit lesions of patients with acute coronary syndromes and lesions in patients without acute coronary syndromes. Circulation 108: 2473-2478.
- Di Vito L, Prati F, Arbustini E, Crea F, Maseri A (2013) A "stable" coronary plaque rupture documented by repeated OCT studies. JACC Cardiovasc Imaging 6: 835-836.
- Yonetsu T, Kakuta T, Lee T, Takahashi K, Kawaguchi N, et al. (2011) In vivo critical fibrous cap thickness for rupture-prone coronary plaques assessed by optical coherence tomography. Eur Heart J 32: 1251-1259.
- Cristell N, Cianflone D, Durante A, Ammirati E, Vanuzzo D, et al. (2011) High-sensitivity C-reactive protein is within normal levels at the very onset of first ST-segment elevation acute myocardial infarction in 41% of cases: a multiethnic case-control study. J Am Coll Cardiol 58: 2654-2661.
- Giannopoulos G, Pappas L, Synetos A, Hahalis G, Raisakis K, et al. (2014) Association of virtual histology characteristics of the culprit plaque with post-fibrinolysis flow restoration in ST-elevation myocardial infarction. Int J Cardiol 174: 678-682.
- Ivanovic M, Rancic M, Rdzanek A, Filipjak KJ, Opolski G, et al. (2013) Virtual histology study of atherosclerotic plaque composition in patients with stable angina and acute phase of acute coronary syndromes without ST segment elevation. Srp Arh Celok Lek 141: 308-314.
- Xie Y, Mintz GS, Yang J, Doi H, Iniguez A, et al. (2014) Clinical outcome of nonculprit plaque ruptures in patients with acute coronary syndrome in the PROSPECT study. JACC Cardiovasc Imaging 7: 397-405.
- Marzilli M, Merz CN, Boden WE, Bonow RO, Capozza PG, et al. (2012) Obstructive coronary atherosclerosis and ischemic heart disease: an elusive link!. J Am Coll Cardiol 60: 951-956.