Research Article
Neerja Puri, MD, FICS, FIMSA, FCGP 1*, and Ashutosh Talwar, MS2
1Department of Dermatology and Venereology, G.G.S. Medical College & Hospital
2General Surgery, Consultant Dermatologist & Surgeon, Punjab Health Systems Corporation
Corresponding author
Dr. Neerja Puri, MD, FICS, FIMSA, FCGP, Dermatology, Anesthesiology, Department of Dermatology and Venereology, G.G.S. Medical College & Hospital , Ludhiana, Punjab, India, Tel: 0091-98146-16427; E-mail: neerjaashu@rediffmail.com
Received Date: 03rd March 2015
Accepted Date: 27th March 2015
Published Date: 30th March 2015
Citation
Puri N, Talwar A (2015) Efficacy of Tattoo Removal with Dermabrasion versus Radiofrequency Ablation in a Resource Limited Setting Enliven: Clin Dermatol 1(1): 001.
Copyright
@ 2015 Dr. Neerja Puri. This is an Open Access article published and distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Introduction:
Cosmetic tattoos have become increasingly popular these days.There are many methods of tattoo removal including dermabrasion, radiofrequency ablation, surgical methods, chemical peels and Qswitchedlasers.In a resource poor setting or in patients who cannot afford lasers, both dermabrasion and radiofrequency ablation work well.
Aims:
To study the efficacy of dermabrasion and radiofrequency ablation for the treatment of tattoos.
Methods:
We selected twenty patients with tattoo for the study. The patients were divided into two groups of ten patients each. In group I patients tattoo removal was done using dermabrader and in group II patients, radiofrequency ablation was done for the removal of tattoos.
Results and Discussion:
More than 80% reduction in tattoo pigment was seen in 50% patients in group I and 40% patients in group II, 51-75% reduction in tattoo pigment was seen in 40% patients in both group I and group II patients, 26-50% reduction in tattoo pigment was seen in 10% patients in group I and 20% patients in group II. Regarding the post procedure complications, hypertrophic scar formation was seen in 10% cases in group I and 5% cases in group II, hyperpigmented skin was seen in 5% cases in both group I and group II, incomplete pigment removal was seen in 5% cases in group I and 10% cases in group II, pain and swelling was seen in 20% cases in group I and 10% cases in group II and acceptable scar formation was seen in 35% cases in group I and 10% cases in group II.
Keywords
Tattoos; Dermabrasion; Radiofrequency; Lasers; Pigments; Lasers
Introduction
The tattoo removal market has boomed over the years following the increased prevalence of tattooed individuals around the world. Surgery and laser are currently the gold standards for tattoo removal [1,2]. However, both of them have drawbacks. Surgery is better suited for small tattoos in areas of adequate skin laxity but leave a scar, while laser removal is a long and painful procedure, with no guarantee of a complete efficacy [3,4]. Both are expensive procedures, and not all individuals are ready to fund them privately. Consequently, some individuals are in the search of faster, easier, and cheaper procedures that can be performed either by themselves or by laypeople [5]. The unregulated market of internet provides a favorable ground for many websites to offer various tattoo removal methods.
Cosmetic tattoos have become increasingly popular these days. There are various techniques of tattoo removal including surgical excision; dermabrasion and lasers.Tattoos can be removed permanently with the help of q- switched Nd-YAG laser [6]. This laser breaks down the tattoo pigment that is then absorbed by the body. Multiple sittings, usually 4-5 are required for complete clearance of the tattoo. Certain tattoo pigments, such as red and yellow are more difficult to treat than the green and black pigment. Usually, there is no pain, scarring or other adverse- effects. Although Q switched lasers are gold standard for tattoo removal, but complete removal may be more difficult in lighter skinned patients and also in older tattoos in which complete removal may not be possible, since some dermal pigment may have penetrated too deeply to be reached. Also, the financial cost of the laser treatment preludes some patients from undergoing such treatments. Laser treatment requires multiple painful sessions that are expensive and sometimes incompletely successful [7,8]. With an increase in the number of ink colors, tattoo removal is becoming increasingly difficult. Historically, removal of undesired tattoos included tissue-destructive techniques such as dermabrasion, cryosurgery, electro-surgery and surgical excision [9-11]. Although effective at removing the tattoo ink, these treatments often led to scarring and unwanted skin pigmentation changes.
Dermabrasion is an effective method of removing unwanted tattoos. But some tattoos are harder to remove than the others [12]. Professional tattoos are more easily removed than the amateur tattoos as amateur tattoos are applied at varying depth underneath the skin [13,14]. In dermabrasion the outer layer of the skin is scraped with a wire brush or a diamond fraise. Dermabrasion stimulates the production and growth of new collagen and skin tissue in which the skin cells are more plentiful and better vascularized. The healing process after dermabrasion is usually complete within two weeks after the procedure, but some redness may be present for upto three months [15]. A temporary burning sensation, itching, redness and swelling can be seen after the procedure. A certain degree of bruising and swelling can be expected following treatment, as well as some bleeding and weeping from the wounds [16]. It should also be noted that the process is very painful, and the area is often left feeling numb or with a tingling sensation. There are various gels and creams which can be applied to sooth the area, and exposure to the sun following the procedure must be avoided [17]. Permanent scarring is common, as well as discolouration of the skin due to the top layers being removed, particularly in people with darker complexions. Great care must be taken to avoid infection as the area will be vulnerable due to the protective top layers of skin having been removed. Those who suffer from or have a history of bleeding disorders or keloidal scars cannot use dermabrasion for tattoo removal. This method is often a last resort for those who have had previous unsuccessful tattoo removal treatments. It is generally a successful method except for the pain and scarring involved in the treatment.
The radiofrequency ablation technique is an approach in which the electromagnetic wave is transmitted via an electrode to vibrate the molecules of the tissues with which it comes into contact [18]. Because only the contacted tissues are ablated, virtually little harm is done to adjacent tissues that are not in contact with the electrode, and thermal conduction to the normal skin is reduced. Another advantage of the intralesional radiofrequency ablation method is that each deep seated lesion can be removed effectively, and the unharmed adjacent normal tissues between each lesion are helpful in achieving a good recovery [19,20]. To conclude, intralesional radiofrequency ablation is an effective, inexpensive, highly precise and safe way of treating. Radiofrequency (RF) surgery involves passage of radio waves at the frequency of 1.5 to 4.5 MHz. In case of skin lesions, the most commonly used frequency is 3.8 MHz.The advantages of radiofrequency include rapid healing, minimal bleeding, quick and used as an office procedure. But, over treatment may produce greater tissue destruction & scarring. To conclude, radio-surgery is a faster evolving technique being effective, simple, quick & cost effective.
Aims
1. To study the efficacy of dermabrasion and radiofrequency ablation for the treatment of tattoos
2. To compare the efficacy between the two treatment modalities.
Material and Methods
We selected twenty patients with tattoo for the study. The patients were divided into two groups of ten patients each. In group I patients tattoo removal was done using dermabrader and in group II patients, radiofrequency ablation was done for the removal of tattoos. Written informed consent was taken from all the patients before the study and prior approval of hospital ethical committee was taken before the study. Before starting with the treatment, proper counselling of the patients was done regarding the pros and cons of both the procedures and was informed well in advance about the development of scar after both the procedures. Both dermabrasion and tattoo removal required 1 â?? 4 sessions depending upon the depth of the pigment. The patients were graded according to the percentage of reduction of tattoo pigment as follows: Grade I â?? Upto 25% reduction in tattoo pigment; Grade II â?? 26%- 50% reduction in pigment; Grade III â?? 51%- 75% reduction in pigment; Grade IV â?? > 80% reduction in pigment.
Inclusion Criteria
1. Patients willing for the surgical procedure
2. Patients with realistic expectations
3. Patients who were not able to afford lasers
Exclusion Criteria
1. Patients on oral anticoagulant drugs
2. Patients with history of keloids
3. Patients with history of bleeding tendency
4. Patients with unrealistic expectations.
Dermabrasion was done under local anaesthesia and the patients were instructed to apply the local anaesthetic cream tetralid an hour before the surgery. The intervals between treatment sessions were about 6 weeks. Diamond fraise was used for dermabrading the tattoo and surrounding normal skin was also dermabraded. To prevent bleeding, adrenaline soaked gauzes were used intraoperatively. After the dermabrasion, antibiotic impregnated Vaseline gauze was applied over the lesion and a pressure dressing was done which was opened after seven days. After that patient was asked to apply silicone gel for a period of three months. For radiofrequency ablation of the tattoo, local anaesthetic cream was applied an hour prior to the procedure and a ball shaped electrode was used for the same (Figure 1). Immediately after treatment, mild swelling and erythema with tiny crusting were seen in the treated lesions. All of the patients tolerated the treatment without undue problems. Postoperatively, patients were instructed to apply a topical antibiotic ointment during the first 3 to 5 days after treatment, to lessen the swelling and minimize any risk of infection. Postoperatively in all patients after radiofrequency ablation, the scab was formed in the focal areas and the time of decrustation was 1 to 5 days. Temporary erythema and hyper pigmentation occurred in the majority of patients and then cleared spontaneously in 2 to 3 months. Post procedure sun protection was given in all the patients to prevent post inflammatory hyperpigmentation.
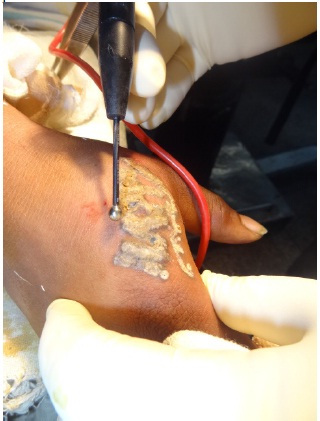
Figure 1 - Figure showing tattoo removal by radiofrequency ablation using a ball shaped electrode
The data was tabulated and the results were analyzed (Table 1- Table 4).
|
Sr no |
Age Distribution of Patients(Years) |
Number |
Percentage |
|
1 |
0 - 20 |
2 |
10% |
|
2 |
21- 40 |
16 |
80% |
|
3 |
41-60 |
2 |
10% |
Table I- Table showing age distribution of patients
|
Sr no |
Cause of Tattoo Removal |
Number |
Percentage |
|
1 |
Regret |
2 |
10% |
|
2 |
Cosmetic |
3 |
15% |
|
3 |
Army recruitment |
14 |
70% |
|
4 |
Social and family reasons |
1 |
5% |
Table 2 â?? Table showing cause of removal of tattoos
|
Sr No |
Percentage Reduction in Tattoo Pigment |
Gp I |
Gp II |
||
|
No of Pts |
% |
No of Pts |
% |
||
|
1 |
>80% |
5 |
50% |
4 |
40% |
|
2 |
51-75% |
4 |
40% |
4 |
40% |
|
3 |
26-50% |
1 |
10% |
2 |
20% |
Table III â?? Table Showing Percentage Reduction in Tattoo Pigment after Multiple Sessions
|
Sr No |
Side Effects |
Number |
Percentage |
||
|
|
|
Gp I |
Gp II |
Gp I |
Gp II |
|
1 |
Hypertrophic scar |
2 |
1 |
10% |
5% |
|
2 |
Hyperpigmented skin |
1 |
1 |
5% |
5% |
|
3 |
Incomplete pigment removal |
1 |
2 |
5% |
10% |
|
4 |
Pain and swelling |
4 |
2 |
20% |
10% |
|
5 |
Acceptable scar formation |
7 |
8 |
35% |
40% |
Table IV - Table Showing Post Procedure Complications
In our study, all the patients who came for tattoo removal were males. Regarding the age distribution of patients, maximum patients (80%) were in the age group of 21-40 years followed by 10% each in the age group of 41-60 years and below 20 years. Commonest cause of tattoo removal in our study was army recruitment (70%), followed by cosmetic reasons (15%), regret was the cause in 10% cases followed by social and family reasons in 5% cases. More than 80% reduction in tattoo pigment was seen in 50% patients in group I (Figure 2 & Figure 3) and 40% patients in group II (Figure 4), 51-75% reduction in tattoo pigment was seen in 40% patients in both group I and group II patients, 26-50% reduction in tattoo pigment was seen in 10% patients in group I and 20% patients in group II. Regarding the post procedure complications, hypertrophic scar formation was seen in 10% cases in group I (Figure 5), and 5% cases in group II, hyperpigmented skin was seen in 5% cases in both group I and group II, incomplete pigment removal was seen in 5% cases in group I and 10% cases in group II, pain and swelling was seen in 20% cases in group I and 10% cases in group II and acceptable scar formation was seen in 35% cases in group I and 10% cases in group II. The residual skin results were excellent with remarkable patient satisfaction. The tattoo features were obscured by the surrounding healed skin. Complete clearance of tattoos was seen in 2- 4 sittings.

Figure 2 - Figure showing tattoo on an arm of a patient before after 3 weeks of dermabrasion (first session)

Figure 3 - Figure showing tattoo on the back of a patient after 3 sessions of dermabrasion
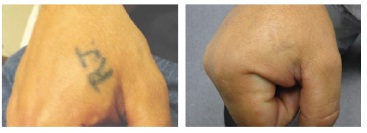
Figure 4- Figure showing tattoo on the hands of a patient before and after 3 sessions of radiofrequency ablation

Figure 5- Figure showing hypertrophic scar formation after tattoo removal by dermabrasion
Tattoo types vary according to aetiology, pigment, depth and purpose. There are five types of tattoos: amateur, professional, cosmetic, medicinal, and traumatic [21]. Poor decision making and subsequent personal regret seem to be frequent motivations for tattoo removal. Important factors to consider when evaluating tattoos for removal are: location, age and the skin type of the patient. We like also to add other important factors related to the tattoo such as: size, form and shape of the tattoo. Cosmetic tattoos often serve to enhance physical features or mask scars. Decorative tattoos can be applied professionally or by amateurs, with pigment initially remaining in the superficial dermis, after several years, the pigment may migrate into the deeper layers of the skin. Amateur tattoos are composed of ink or carbon; these pigments are usually less dense than those used by the professionals, often making amateur tattoos easier to remove. Professional tattoos are composed of organic pigments that vary in particle size but are applied at a uniform depth of needle penetration.
Methods of tattoo removal have been reported since antiquity. Reasons and motivations for tattoo removal have been widely explored. They mainly include social pressure, personal reasons or more simply boredom and dissatisfaction with the tattoo either because it was performed in haste or at a young age or because the result is unaesthetic [22,23]. More rarely, tattoo removal is the last solution in case of severe chronic and refractory local tattoo reaction [24]. Currently, the most efficient treatment, insuring complete pigment removal, is the surgical excision in toto of the tattooed area. The complications are those of any surgical procedure, including mainly the risk of unaesthetic, hypertrophic, or keloid scar [25]. The other gold standard technique is laser removal using either ablative CO2, Q-switched lasers. However, the procedure is long, painful, and the number of sessions is unpredictable. Complete removal is never guaranteed even in expert hands. Laser removal may also lead to complications, mainly dyspigmentation and textural changes due to the use of wrong devices or parameters [26-28]. Lastly, this procedure is expensive. The choice of the removal procedure will depend on the availability of each technique in the area, the tattoo itself (type, color, location, size, etc.), and the wishes and expectations of the patient. Dermabrasion removes the layers of the skin on the tattooed area containing ink and let the skin regenerate so that the tattoo is no longer visible. As the ink from most tattoos can be deeply embedded in the layers of the dermis, the dermabrasion process can lead to permanent scars. Dermabrasion tattoo removal should be carried out by a plastic or a cosmetic surgeon with adequate skill in the field. Laser removal of tattoos is not generally or readily available to the public and removal in privately run clinics is expensive. Limitations to laser treatment include the need for multiple treatment sessions, minimal to incomplete responses in some cases, and the possibility of pigment and textural changes with higher cost to the patient. Also, for those seeking removal of their tattoo this can create significant financial hardship. Chemical and surgical methods of tattoo removal usually associated with scars complications Regular dermabrasion method usually gives satisfactory results. Once used in an appropriate clinical setting, dermabrasion provides relatively efficacious clearance of decorative tattoo pigment. However, the shape of the tattoo following dermabrasion may still persist despite lacking some pigments.
In a study conducted by J Muhammad [29], male patients with decorative skin tattoos who underwent layered dermabrasion, the success rate was remarkable with high satisfaction rate by all patients with post operative hypertrohic scarring rate less than 9%.
Conclusions
To conclude, both dermabrasion and radiofrequency ablation are cost effective methods for tattoo removal. It is important that dermabrasion be done only by a plastic surgeon or a trained dermatologist having expertise in this field. Dermabrasion if done with adequate postoperative scar skin care treatment results in complete removal of the tattoo with minimal scaring of the skin. It is a promising method for treating of decorative skin tattoos. Patient counselling is very important before both the procedures and the patient should be properly explained the risks of scar formation.
References
- Milroy BC (1993) Tattoos and their removal. Med J Aust 159: 717-719.
- Lindsay DG (1989) Tattoos. Dermatol Clin 7: 147-153.
- Veysey E, Downs AM (2004) Adverse side-effects following attempted removal of tattoos using a non-laser method. Br J Dermatol 150: 770-771.
- Choudhary S, Elsaie ML, Leiva A, Nouri K (2010) Lasers for tattoo removal: a review. Lasers Med Sci 25: 619-627.
- Kluger N (2010) Tattoo removal at the start of the 20th century. Ann Dermatol Venereol 137: 582-584.
- Troilius AM (1998) Effective treatment of traumatic tattoos with a Q-switched Nd: YAG laser. Lasers Surg Med 22: 103-108.
- Bernstein EF (2006) Laser treatment of tattoos. Clin Dermatol 24: 43-55.
- Mariwalla K, Dover JS (2006) The use of lasers for decorative tattoo removal. Skin Therapy Lett 11: 8-11.
- Dvir E, Hirshowitz B (1980) Tattoo removal by cryosurgery. Plast Reconstr Surg 66: 373-379.
- Boo-Chai K (1963) The Decorative Tattoo: Its Removal by Dermabrasion. Plast Reconstr Surg 32: 559-563.
- Buncke HJ Jr, Conway H (1957) Surgery of decorative and traumatic tattoos. Plast Reconstr Surg 20: 67-77.
- Clabaugh WA (1975) Tattoo removal by superficial dermabrasion. Five-year experience. Plast Reconstr Surg 55: 401-405.
- Aslam A, Owen CM (2013) Fashions change but tattoos are forever: time to regret. Br J Dermatol 169: 1364-1366.
- Sweeney SM (2006) Tattoos: a review of tattoo practices and potential treatment options for removal. Curr Opin Pediatr 18: 391-395.
- Cronin ED, Haber JL (1996) A new technique of dermabrasion for traumatic tattoos. Ann Plast Surg 36: 401-402.
- Peris Z (2002) Removal of traumatic and decorative tattoos by dermabrasion. Acta Dermato-venerol Croat 10: 15-19.
- Hagerman RD, Cranmer LG, Bartok WR, Wilson JW (1970) Topical medications on dermabraded tattoos. Arch Dermatol 102: 438-439.
- Penoff JH (1987) The office treatment of tattoos: a simple and effective method. Plast Reconstr Surg 79: 186-191.
- Bailey BN (1967) Treatment of tattoos. Plast Reconstr Surg 40: 361-371.
- Varma S, Lanigan SW (1999) Reasons for requesting laser removal of unwanted tattoos. Br J Dermatol 140: 483-485.
- Apfelberg DB, Manchester GH (1987) Decorative and traumatic tattooremoval. Clin Plast Surg 14: 243-251.
- Armstrong ML, Roberts AE, Koch JR, Saunders JC, Owen DC, et al. (2008) Motivation for contemporary tattoo removal: a shift in identity. Arch Dermatol 144: 879-884.
- Latreille J, Levy JL, Guinot C (2011) Decorative tattoos and reasons for their removal: a prospective study in 151 adults living in South of France. J Eur Acad Dermatol Venereol 25: 181-187.
- Koljonen V, Kluger N (2012) Specifically requesting surgical tattoo removal: are deep personal motivations involved? J Eur Acad Dermatol Venereol 26: 685-689.
- Hudson DA, Lechtape-Gruter RU (1990) A simple method of tattoo removal. S Afr Med J 78: 748-749.
- Lanigan SW, Sheehan-Dare RA, Cotterill JA (1989) The treatment of decorative tattoos with the carbon dioxide laser. Br J Dermatol 120: 819-825.
- Suchin KR, Greenbaum SS (2004) Successful treatment of a cosmetic tattoo using a combination of lasers. Dermatol Surg 30: 105-107.
- Kent KM, Graber EM (2012) Laser tattoo removal: a review. Dermatol Surg 38: 1-13.
- Mohammad J (2006) Layered Dermabrasion: A Simple Controlled Method for the Treatment of Tattoos. The Internet Journal of Plastic Surgery 3: 1-2.