Original Research
Mohammad M. Abd-Alhaseeb1*, Sawsan A. Zaitone2, Soad H. Abou-El-Ela3, and Yasser M. Moustafa2
1Department of Pharmacology and Toxicology, Faculty of Pharmacy and Pharmaceutical Industries, Sinai University, Arish, Egypt
2Department of Pharmacology and Toxicology, Faculty of Pharmacy, Suez Canal University, Ismailia, Egypt
3Department of Biochemistry, Faculty of Pharmacy and Pharmaceutical Industries, Sinai University, Arish, Egypt
Corresponding author
Mohammad M. Abd-Alhaseeb, Department of Pharmacology and Toxicology, Faculty of Pharmacy and Pharmaceutical Industries, Sinai University, Arish, Egypt, Tel: 002-010-07699126; Fax: 002-068-3336847; E-mail: m.abdelhasseb@su.edu.eg
Received Date: 06th August 2014
Accepted Date: 08th September 2014
Published Date: 12th September 2014
Citation
Abd-Alhaseeb MM, Zaitone SA, Abou-El-Ela SH, Moustafa YM (2014) Angiotensin (1-7) Antagonist Diminished the Anti-Tumor Effect of Olmesartan in Tumor Cell Lines Grown In-vitro and In-vivo. Enliven: Challenges Cancer Detect Ther 1(1): 003.
Copyright
@ 2014 Dr. Mohammad M. Abd-Alhaseeb. This is an Open Access article published and distributed under the terms of the Creative Commons Attribution License, that permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Olmesartan is a selective angiotensin II type 1 receptor (AT1R) antagonist. It achieves blood pressure reduction in a dose-dependent manner through arterial vasodilation and reduced sodium retention. Secondly, olmesartan exhibits anti-angiogenic activity through inhibition of Insulin growth factor, vascular endothelial growth factor and their receptors and this effect was mediated through the Ang (1-7). The current study was to investigate the anti-tumor effect of olmesartan; first, the cytotoxic activity of olmesartan and/or Ang (1-7) antagonist on MCF-7 cell line using 3-[4, 5-dimethylthiazole-2-yl]-2, 5-diphenyltetrazolium bromide (MTT) assay was explored. Then EAC solid tumor grown in vivo was employed to determine the impact of concurrent administration of an Ang (1–7) agonist or antagonist on the anti-tumor effect of olmesartan. In addition, the impact of concurrent administration of olmesartan on the cytotoxic activity of sorafenib in MCF-7 cell line or its anti-tumor effect in EAC solid tumor grown in vivo was investigated. It was observed that the cell viability was reduced by approximately 40% after sorafenib (250 μg/ml) treatment. On the other hand, olmesartan did not show any cytotoxic effect except when higher concentrations were used. IC50 value for sorafenib in MCF-7 was 250.9 μg/ml, while the IC50 value for olmesartan was 674.8 μg/ml. Ang (1-7) antagonist increased the IC50 value of olmesartan from 674.8 μg/ml to 722 μg/ml. The high cytotoxic concentration of olmesartan in combination with sorafenib failed to enhance the cytotoxicity more than the sorafenib itself. Sorafenib (30 mg/kg/day), olmesartan (3, 10 or 30 mg/kg/day) or their combination significantly (P<0.05) reduced tumor volume and the relative tumor volume compared to EAC-Control group. Similarly, concurrent administration of the Ang (1-7) agonist with olmesartan (30 mg/kg) significantly (P<0.05) reduced tumor volume and the relative tumor volume compared to EAC-control group or olmesartan (30 mg/kg) group. Moreover, the administration of Ang (1-7) antagonist with olmesartan reduced the anti-tumor effect of olmesartan. In conclusion, olmesartan (30 mg/kg) posses anti-tumor activity. This anti-tumor activity did not depend on the direct cytotoxic activity but might be attributed to antiangiogenic activity as proven in a previous work from our lab. The anti-tumor effect of olmesartan was, at least in part, mediated through the Ang (1-7) receptor. In addition, the present results showed that olmesartan (30 mg/kg) potentiated the anti-tumor effect of sorafenib.
Abstract
Olmesartan is a selective angiotensin II type 1 receptor (AT1R) antagonist. It achieves blood pressure reduction in a dose-dependent manner through arterial vasodilation and reduced sodium retention. Secondly, olmesartan exhibits anti-angiogenic activity through inhibition of Insulin growth factor, vascular endothelial growth factor and their receptors and this effect was mediated through the Ang (1-7). The current study was to investigate the anti-tumor effect of olmesartan; first, the cytotoxic activity of olmesartan and/or Ang (1-7) antagonist on MCF-7 cell line using 3-[4, 5-dimethylthiazole-2-yl]-2, 5-diphenyltetrazolium bromide (MTT) assay was explored. Then EAC solid tumor grown in vivo was employed to determine the impact of concurrent administration of an Ang (1?7) agonist or antagonist on the anti-tumor effect of olmesartan. In addition, the impact of concurrent administration of olmesartan on the cytotoxic activity of sorafenib in MCF-7 cell line or its anti-tumor effect in EAC solid tumor grown in vivo was investigated. It was observed that the cell viability was reduced by approximately 40% after sorafenib (250 ?g/ml) treatment. On the other hand, olmesartan did not show any cytotoxic effect except when higher concentrations were used. IC50 value for sorafenib in MCF-7 was 250.9 ?g/ml, while the IC50 value for olmesartan was 674.8 ?g/ml. Ang (1-7) antagonist increased the IC50 value of olmesartan from 674.8 ?g/ml to 722 ?g/ml. The high cytotoxic concentration of olmesartan in combination with sorafenib failed to enhance the cytotoxicity more than the sorafenib itself. Sorafenib (30 mg/kg/day), olmesartan (3, 10 or 30 mg/kg/day) or their combination significantly (P < 0.05) reduced tumor volume and the relative tumor volume compared to EAC-Control group. Similarly, concurrent administration of the Ang (1-7) agonist with olmesartan (30 mg/kg) significantly (P < 0.05) reduced tumor volume and the relative tumor volume compared to EAC-control group or olmesartan (30 mg/kg) group. Moreover, the administration of Ang (1-7) antagonist with olmesartan reduced the anti-tumor effect of olmesartan. In conclusion, olmesartan (30 mg/kg) posses anti-tumor activity. This anti-tumor activity did not depend on the direct cytotoxic activity but might be attributed to antiangiogenic activity as proven in a previous work from our lab. The anti-tumor effect of olmesartan was, at least in part, mediated through the Ang (1-7) receptor. In addition, the present results showed that olmesartan (30 mg/kg) potentiated the anti-tumor effect of sorafenib.
Keywords:
Anti-tumor; Angiotensin (1-7) antagonist; Olmesartan; Cancer; Cell line
Introduction
The Renin-angiotensin system (RAS) is a hormone system that is activated when the enzyme renin is released and cleaves the parent compound angiotensinogen to the decapeptide angiotensin I (Ang I). The catabolism of Ang I is a point of divergence in the system, leading to the production of the bioactive peptide hormones, angiotensin II (Ang II) and angiotensin (1-7) (Ang (1-7)). These peptide products differ in their carboxy termini which leads to counter-regulatory actions mediated by high affinity binding to distinct membrane-spanning receptors [1].
Ang (1-7) exerts its actions through a G protein-coupled receptor encoded by the mas gene [2]. Ang (1?7) appears to have an inhibitory influence on many of the events induced by Ang II [3]. Ang (1?7) has a depressor, vasodilator, apoptotic and anti-proliferative actions. Ang (1?7) was suggested to inhibit angiogenesis [4], although further investigations are needed to confirm these effects in a wider range of pathological/physiological conditions.
Ang (1?7) may be generated directly from Ang II by the enzymatic activity of angiotensin converting enzyme two (ACE2) or from Ang I, via angiotensin (1?9), a pathway that utilizes both ACE2 and angiotensin converting enzyme (ACE) [5]. ACE2 was found in many tissues with high concentrations in the heart, kidney and gastrointestinal tract [6]. In addition, ACE2 expression was reported in animal models of liver injury and in human cirrhosis and was associated with increasing plasma and tissue levels of Ang (1?7) [7].
Olmesartan is a selective angiotensin II type 1 receptor (AT1R) antagonist. It achieves blood pressure reduction in a dose-dependent manner through arterial vasodilation and reduced sodium retention [8]. In addition, olmesartan exhibits anti-angiogenic activity through inhibition of Insulin growth factor, vascular endothelial growth factor and their receptors and this effect was mediated through the Ang (1-7) [9]. Sorafenib is a multi-kinase inhibitor taken orally and approved in the treatment of metastatic renal cell carcinoma [10]. It has been reported that olmesartan potentiated the anti-angiogenic effect of sorafenib in Ehrlich?s ascites carcinoma (EAC) solid tumor grown in vivo in mice [9]. So, the objective of the current study was to investigate the anti-tumor effect of olmesartan; beginning with exploring the cytotoxic activity of olmesartan and/or Ang (1-7) antagonist on MCF-7 cell line using 3-[4, 5-dimethylthiazole-2-yl]-2, 5-diphenyltetrazolium bromide (MTT) assay. Then, EAC solid tumor grown in vivo was employed to determine the impact of concurrent administration of an Ang (1?7) agonist or antagonist on the anti-tumor effect of olmesartan. Finally, investigate the impact of concurrent administration of olmesartan on the cytotoxic activity of sorafenib in MCF-7 cell line or its anti-tumor effect in EAC solid tumor grown in vivo.
Methods and Materials
Cell Culture and Drug Treatment
The MCF-7 human breast adenocarcinoma cell line was purchased from American Type Culture Collection (ATCC, Manassas, VA, USA). It was maintained in Dulbecco's Modified Eagle's Medium containing 10% fetal bovine serum, 100 units/mL penicillin, and 100 mg/mL streptomycin. Cells were incubated in a humidified, 5% CO2 atmosphere at 37°C.
MTT Assay for Cell Viability
MTT assay is based on the ability of active mitochondrial dehydrogenase enzyme of living cells to cleave the tetrazolium rings of the yellow MTT and form dark blue insoluble formazan crystals which is largely impermeable to cell membranes, resulting in its accumulation within healthy cells. The effect of olmesartan and/or sorafenib and Ang (1-7) antagonist on cell viability was determined using MTT assay. In MTT assay 0.5×105 cells per well were plated in 96-well culture plates. After an overnight incubation, cells were treated with 20 ?l of different concentrations of olmesartan and/or sorafenib for 48 h at 37°C. The cells were then treated with 40 ?l of MTT (Sigma-Aldrich, MO, USA) and Incubated for 4 h at 37°C. The medium was then discarded, and 180 ?l of acidified isopropanol (Sigma-Aldrich, MO, USA) was added to dissolve formazan crystals.
Absorption values at 570 nm were determined with Multiskan MS microplate reader (Labsystems, Finland). The cell viability of olmesartan and/or sorafenib-treated cells was calculated as the percentage of cell viability compared to untreated cells. In addition, IC50 values were calculated from the equation of the curve.
Anti-Tumor Activity of Olmesartan and/or Sorafenib in Ehrlich?s Ascites Carcinoma Solid Tumor Grown in Mice
Female Swiss albino mice, each weighing 20-25 g were obtained from the modern veterinary office for laboratory animals (Cairo, Egypt). EAC cell line was purchased from Tumor Biology Department, National Cancer Institute (Cairo University, Egypt). EAC cells were injected intradermally (2.5 × 106 EAC cells in 0.1 ml saline/animal) at the two sites bilaterally on the lower ventral side after shaving this area. After 7 days, mice were randomly divided into eight groups, ten animals each.
All treatments were given for 21 days and the treatment regimens were as follows: Group I: mice treated with DMSO (5 mL/kg/day, p.o.), and served as the EAC-control group. Group II: mice treated with sorafenib (30 mg/kg/day, p.o.) [11]. Group III-V: mice treated with olmesartan (3, 10 or 30 mg/kg/day, p.o.), respectively [12]. Group VI: mice treated with a combination of sorafenib (30 mg/kg/day, p.o.) and olmesartan (30 mg/kg/day, p.o.). Group VII: mice treated with olmesartan (30 mg/kg/day, p.o.) and the angiotensin (1-7) agonist (30 ?g/kg/day, i.p.) [13]. Group VIII: mice were treated with olmesartan (30 mg/kg/day, p.o.) and the angiotensin (1-7) antagonist (A-779 peptide) (3.3 mg/kg/trice weekly, i.p.) [14]. In general, olmesartan and sorafenib were administered daily by gastric gavage in a volume of 5 mL/kg. Whereas, the angiotensin (1-7) agonist or the angiotensin (1-7) antagonist were administered intraperitoneally.
At the end of the experiment, the animals were sacrificed with cervical dislocation. The tumors were separated from the surrounding muscles and dermis; tumor volumes were measured with vernier calipers and calculated by the following formula: 0.5 X2Y, where X and Y are the minor and major axes, respectively [15]. In addition, the relative tumor volumes were calculated by dividing the mean tumor volumes of the treated groups by the mean tumor volume of the control group [16]. All experimental protocols were approved by The Research Ethics Committee at the Faculty of Pharmacy, Suez Canal University (License number 20146A10).
Drugs and Chemicals
Olmesartan medoxomil was obtained from Daiichi Sankyo Pharmaceutical Co. (Tokyo, Japan) and dissolved at a concentration of 100 mM in dimethyl sulphoxide (DMSO, Sigma-Aldrich, MO, USA) as a stock solution. It was then further diluted to working concentrations with cell culture medium in in-vitro study and with water in in-vivo study. Sorafenib tosylate was purchased from Bayer Health Care (Leverkusen, Germany). Ang (1-7) agonist and antagonist were purchased from Bachem AG (Bubendorf, Zurich, Switzerland). All other chemicals were purchased from Sigma-Aldrich (MO, USA).
Statistical Analysis
In-vitro results were expressed as mean ± standard deviation (SD). Results were analysed in terms of IC50 values, and differences noted across the cell-line panel and within individual cell lines were tested for statistical significance using Chi-square test. On the other hand data from in-vivo results were expressed as mean ± standard error of mean (SEM) and was analyzed using one-way analysis of variance (ANOVA), followed by Bonferroni?s post hoc test at P<0.05. Statistical analysis was performed using SPSS software, version 22 (SPSS Software, SPSS Inc., Chicago, USA).
Results
Effect on MCF-7 Cell Line
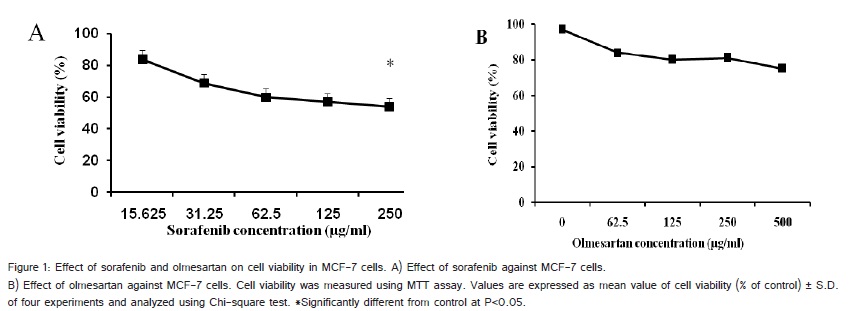
First, we determined the cytotoxic effect of sorafenib and olmesartan on MCF-7 breast cancer cells using MTT assay. MCF-7 cells were treated with various concentrations of sorafenib and olmesartan. After sorafenib treatment, cell viability was reduced by approximately 40% (Figure 1A). On the other hand, olmesartan did not show any cytotoxic effect except when higher concentrations were used (Figure 1B).
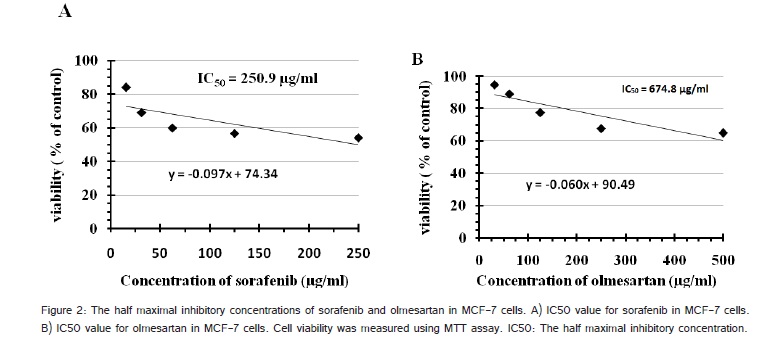
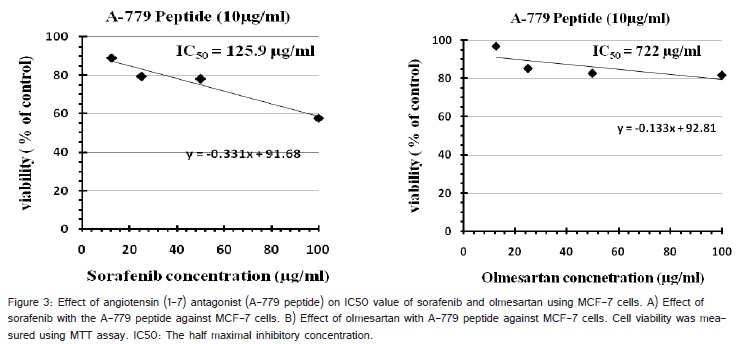
IC50 value for sorafenib in MCF-7 was 250.9 ?g/ml, while the IC50 value for olmesartan was 674.8 ?g/ml (Figure 2A and 2B). On the other hand, the Ang (1-7) antagonist (A-779 peptide) showed a safe effect on the same cell line up to 50 ?g/ml, so that the used concentration (10 ?g/ml) was completely safe with viability percent > 85%.
In the low concentration range up to 100 ?g/ml of sorafenib or olmesartan, the 10 ?g/ml of peptide decreased the IC50 of sorafenib from 250.9 ?g/ml to 125.9 ?g/ml. On the other hand, the peptide (10 ?g/ml) treatment in combination with olmesartan increased the IC50 value from 674.8 ?g/ml to 722 ?g/ml (Figure 3A and 3B).
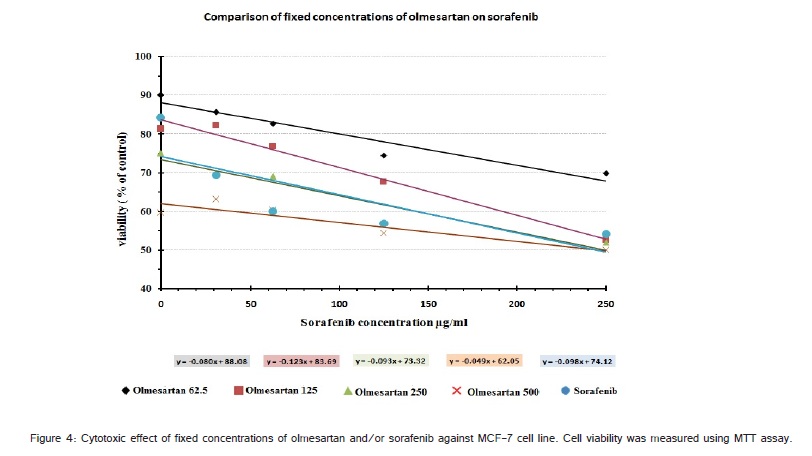
The combination of olmesartan and sorafenib, with different concentrations of both, showed different effects (Figure 4). Olmesartan itself at highest used concentration (500 ?g/ml) - without sorafenib - enhanced cytotoxicity from about 90% of cell viability - at olmesartan concentration 62.5 ?g/ml - into only 60% of cell viability. However such high cytotoxic concentration of olmesartan in combination with sorafenib failed to enhance the cytotox icity more than the sorafenib itself (Figure 4).
Effect on Tumor Volume
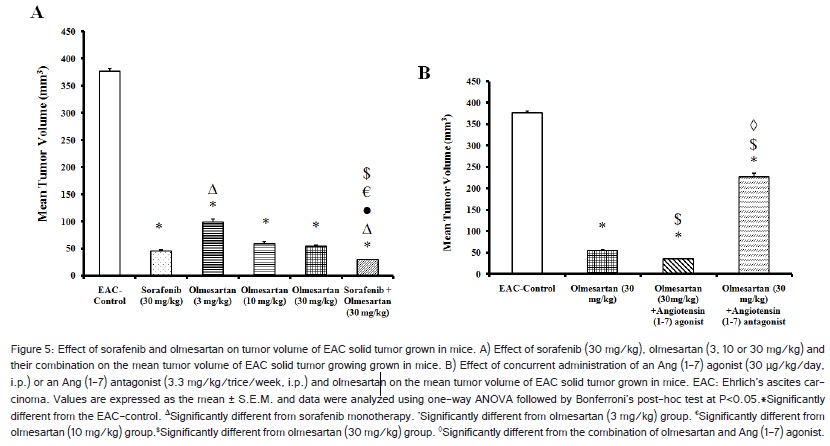
Administration of sorafenib (30 mg/kg/day), olmesartan (3, 10 or 30 mg/kg/day) or their combination significantly (P < 0.05) reduced tumor volume compared to EAC-Control group (Figure 5A). Similarly, concurrent administration of the Ang (1-7) agonist with olmesartan (30 mg/kg) significantly (P < 0.05) reduced tumor volume compared to EAC-control group or olmesartan (30 mg/kg) group. Moreover, the administration of Ang (1-7) antagonist with olmesartan reduced the antitumor effect of olmesartan (Figure 5B).
Effect on the Relative Tumor Volume
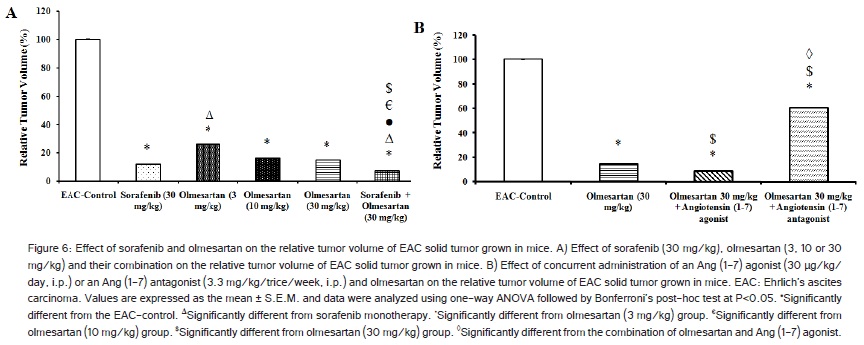
The administration of sorafenib (30 mg/kg/day), olmesartan (3, 10 or 30 mg/kg/day) or their combination showed a significant (P< 0.05) decrease in the % relative tumor volume when compared to EAC-control group (Figure 6A). Similarly, concurrent administration of the Ang (1-7) agonist with olmesartan (30 mg/kg) significantly (P < 0.05) reduced the % relative tumor volume compared to EAC-Control group or olmesartan (30 mg/kg) group. Further, the administration of Ang (1-7) antagonist with olmesartan reduced the antitumor effect of olmesartan (Figure 6B).
Discussion
There are increasing evidences for in-vivo and in-vitro models of angiogenesis indicating a regulatory role of Ang II and its receptors in new vessel formation [17]. Ang II has been reported to promote tumor growth and angiogenesis [18]. Therefore, angiotensin receptor blockers have been considered a noteworthy anticancer and anti-angiogenesis therapeutic option [18].
Angiotensin II type 1 receptor is often up-regulated during the progression from normal to malignant phenotypes, indicating at the very least a correlation between the RAS and tumour progression [3]. Therefore, AT1R blockers have been considered as an anti-angiogenic therapeutic option [19].
Ang (1?7) appears to have an inhibitory influence on many of the events induced by Ang II [3]. Ang (1?7) has a depressor, vasodilator, apoptotic and anti-proliferative actions. Ang (1?7) is also suggested to inhibit angiogenesis [4].
In the current study, olmesartan showed a cytotoxic activity and reduced the cell viability of MCF-7 cells with IC50 value of 675 ?g/ml; however this is considered a high cytotoxic concentration. Therefore, we suggested that the anti-tumor effect of olmesartan is not a result of direct toxicity. Consistently, it has been reported that the antitumor effect of ARBs is not a result of direct toxicity but of an anti-angiogenic effect [20,21]. In addition, it has been reported that in the MCF-7 cell line, Ang II increased the basal protein kinase activity and so increased growth of MCF-7 cells. Consequently, ARBs decreased growth of MCF-7 cells through inhibition of protein kinase activity not due to cytotoxic activity [22]. Another study came in parallel with the present findings as candesartan, type of ARBs, did not induce direct cytotoxicity in in-vitro human bladder cancer cells [20].
In addition, the current results demonstrated that the Ang (1-7) antagonist increased the IC50 value of olmesartan indicated the antagonist effect exerted by the Ang (1-7) antagonist on olmesartan. In agreement with the previous results, it has been reported that the specific Ang (1?7) receptor antagonist (A-779 peptide) prevented the effects of ARBs and Ang (1?7) itself [4].
On the other hand, sorafenib showed a higher cytotoxic activity against MCF-7 cell lines with IC50 value of 250 ?g/ml; that indicated the higher cytotoxicity of sorafenib over olmesartan. In agreement with the previous results, it has been reported that sorafenib showed a broad cytotoxic activity against various tumor cell lines in-vitro and in xenograft models [23].
Additionally, the current study showed that olmesartan at the highest used concentration (500 ?g/ml) enhanced cytotoxicity from about 90% of cell viability into only 60% of cell viability. Therefore, olmesartan showed a little cytotoxic activity. In agreement with the previous results, it has been reported that the ARBs showed a mild cytotoxic activity on tumor cell lines [21].
This is the first time to examine the cytotoxic effect of olmesartan and/or sorafenib on MCF-7 cells. The current results showed that the highest cytotoxic concentration of olmesartan in combination with sorafenib failed to enhance the cytotoxicity more than the sorafenib itself indicating no in-vitro synergistic effect in the cytotoxicity between the two compounds despite of the toxicity of each one separately.
The in-vivo anti-tumor activity of olmesartan was evaluated in the present study by determination of tumor volume and the relative tumor volume in EAC solid tumor grown in mice. The current study showed that olmesartan reduced the tumor volume and relative tumor volume assuming that this was linked to the angiostatic effect of olmesartan which resulted in tumor growth impairment. In agreement with the previous results, it has been reported that candesartan reduced tumor volume in a xenograft model of bladder cancer [20].
Furthermore, consistently with the previous results losartan reduced cell growth of in-vivo models of cancer [24]. Also, telmisartan, caused marked inhibition of prostate cancer cells in concentration-dependent and time-dependent manner [18].
The current results showed that the combination of olmesartan (30 mg/kg) with the Ang (1-7) agonist reduced the tumor volume and the relative tumor volume. On the other hand, the Ang (1-7) antagonist (A-779 peptide) antagonized the anti-tumor effect of olmesartan. Therefore, we suggested that the anti-tumor effect of olmesartan is mediated through the Ang (1-7) receptors. In agreement with the previous results it has been reported that the Ang (1-7) antagonist antagonized the anti-tumor effect of Ang (1-7) agonist and ARBs in human lung cancer cell model [25].
The current study also showed that sorafenib reduced tumor volume and the relative tumor volume. In agreement with the previous results, it has been reported that sorafenib reduced tumor size and tumor weight in hepatocellular carcinoma [26]. In addition, it has been reported that sorafenib reduced tumor weight and tumor volume in neuroblastoma model of cancer [27]. Another study came in parallel with the results in the current study, it showed that sorafenib reduced tumor weight in human liver cancer model [28].
Moreover, the current study showed that olmesartan (30 mg/kg) potentiated the anti-tumor effect of sorafenib. The combined therapy reduced tumor volume and the relative tumor volume and this effect was attributed to the anti-angiogenic effect of the combined therapy. Similarly, it has been reported in previous study that the combined therapy of olmesartan and sorafenib produced an anti-angiogenic activity that was confirmed by reducing tumor weight of EAC solid tumor grown on mice [9].
Conclusion
In conclusion, the present results showed that olmesartan (30 mg/kg) posses anti-tumor activity. This anti-tumor activity did not depend on the direct cytotoxic activity but might be attributed to antiangiogenic activity as proven in a previous work from our lab. The anti-tumor effect of olmesartan was, at least in part, mediated through the Ang (1-7) receptor. In addition, the present results showed that olmesartan (30 mg/kg) potentiated the anti-tumor effect of sorafenib. Therefore, the present study highlights the beneficial role of olmesartan as an adjuvant medication to sorafenib in the treatment of cancer.